Print Entire Issue
.jpg)

Illinois Council of Health-System Pharmacists
4055 North Perryville Road
Loves Park, IL 61111-8653
Phone: (815) 227-9292
Fax: (815) 227-9294
ichpnet.org
KeePosted
Official News journal of the Illinois Council of Health-System Pharmacists
EDITOR
Jennifer Phillips
ASSISTANT EDITOR
Milena Murray
MANAGING EDITOR
Trish Wegner
ASSISTANT MANAGING EDITOR
Maggie DiMarco Allen
DESIGN EDITOR
Melissa Dyrdahl
ICHP Staff
EXECUTIVE VICE PRESIDENT
Chris Crank
VICE PRESIDENT - PROFESSIONAL SERVICES
Trish Wegner
DIRECTOR OF OPERATIONS
Maggie Allen
INFORMATION SPECIALIST
Heidi Sunday
CUSTOMER SERVICE AND
PHARMACY TECH TOPICS™ SPECIALIST
Jo Ann Haley
ACCOUNTANT
Kim Anderson
COMMUNICATIONS MANAGER
Melissa Dyrdahl
LEGISLATIVE CONSULTANTS
Liz Brown Reeves
ICHP's Mission Statement
Advancing Excellence in
Pharmacy
ICHP's Vision Statement
ICHP dedicates itself to
achieving a vision of pharmacy practice where:
·
Pharmacists are
universally recognized as health care professionals and essential providers of
health care services.
·
Pharmacists use their
medication expertise and leadership skills to optimize the medication use
process and patient outcomes.
·
Pharmacy technicians are
trained and PTCB certified to manage the medication distribution process.
ICHP's Goal Statements
·
Raising awareness of the
critical role pharmacists fulfill in optimizing medication therapy and ensuring
medication safety in team-based, patient-centered care.
·
Providing high quality
educational services through innovative continuing pharmacy education and
training programs, and sharing evidence-based best practices.
·
Developing and nurturing
leaders through mentorship, skill development programs, and leadership
opportunities.
·
Working with national
and state legislators and policymakers to create or revise legislation and
regulation critical to pharmacy practice and quality patient care.
·
Urging pharmacy
technician employers to require successful completion of an accredited pharmacy
technician training program and PTCB certification of all pharmacy technicians.
Approved by the ICHP
Board of Directors May 30, 2018.
KeePosted Vision
As an integral publication of the Illinois Council of Health-System
Pharmacists, the KeePosted newsjournal will reflect its
mission and goals. In conjunction with those goals, KeePosted will
provide timely information that meets the changing professional and personal
needs of Illinois pharmacists and technicians, and maintain high publication
standards.
KeePosted is an official publication of, and is copyrighted by, the
Illinois Council of Health-System Pharmacists (ICHP). KeePosted is
published 4 times a year. ICHP members received KeePosted as
a member benefit. All articles published herein represent the opinions of the
authors and do not reflect the policy of the ICHP or the authors’ institutions
unless specified. Advertising inquiries can be directed to ICHP office at the
address listed above. Image disclaimer: The image used in the Pharmacy Tech
Topics™ advertisement is the property of © 2017 Thinkstock, a division of Getty
Images. Some images are property of © 2021 Adobe Stock.
Copyright © 2021, Illinois Council of Health-System Pharmacists. All rights
reserved.
Columns
President's Message
Crank's Corner
ICHPeople
Board of Pharmacy Update
Government Affairs Report
New Practitioners Network
PEARLS: Public Education & Awareness Outreach Publication Subcommittee
ICHP Leadership Spotlight
ICHP Leadership Spotlight
Professional Affairs
Educational Affairs
Educational Affairs
ICHP Best Practice Award
Features
PTCB Credentials & Certificates
Nominations Committee
Recognize The Best
Spring Meeting Recap
Spring Meeting 2021: Poster & Platform Winners
College Connection
Midwestern University College of Pharmacy, Downers Grove
Southern Illinois University Edwardsville School of Pharmacy
University of Illinois Chicago College of Pharmacy
More
Upcoming Events
Welcome New Members!
ICHP Pharmacy Action Fund Contributors
ICHP Board of Directors 2021-2022
Columns
 150x150.jpg) President's Message
President's Message
Working on Well-Being
by Jennifer Arnoldi, PharmD, BCPS Clinical Associate Professor, SIUE School of Pharmacy President of ICHP
At this year’s Spring Meeting, I presented a poster detailing a research project I completed with a pharmacy student prior to the start of the pandemic. We focused on the issue of burnout in Illinois pharmacists, gathering data from members of ICHP and IPhA. The results were disheartening, showing many pharmacists who responded to the survey were affected by burnout, which encompasses exhaustion and disengagement from work. Pharmacist burnout can have a negative impact on patient care, outcomes, and efficacy at work.1
Along with the increased focus on professional burnout, there has been a growing interest in the topics of mindset, well-being, mindfulness, and resilience. As many of us fulfill caregiver roles at work and at home, this makes perfect sense. What do they tell us to do when there is an unexpected issue on an airplane? Put on your oxygen mask before you assist others. In terms of well-being, we need to put on our oxygen masks and care for ourselves so that we can optimally care for others. In the November 2020 issue of KeePosted, Executive Vice President Chris Crank extolled the virtues of positive thinking, especially during times of stress.2 If you missed “Crank’s Corner” from that issue, I’d encourage you to go back to the archives and give it a read. In our already busy lives, how can we make time for well-being?
One approach is to create a culture of well-being at the workplace. One way is to consider well-being challenges. Consider selecting a monthly well-being focus for the department and find a way to make it competitive. A recent study highlighted well-being challenges created for pharmacy students that focused on smartphone usage, practicing gratitude, achieving good sleep habits, and working on daily movement such as taking a walk.3 It might be necessary to use the honor system to report staff participation in these challenges, but rewards like a small gift card to a local shop or workplace incentives might have an impact. Another suggestion is to implement a weekly focus; my workplace has a “Wellness Wednesday” that has a different topic each week.
Would you rather use an app for that? We have a wealth of them at our fingertips to help us on our well-being journey. Did you know that if you are a member of ASHP that you already have free access to an app called Headspace? It is one of the most popular well-being apps that can help you with meditation, mindfulness, and sleep. This link
https://bit.ly/30kvtmb will help you verify your ASHP account and add this member benefit. Not an ASHP member? If you don’t mind paying a subscription fee, you can purchase Headspace on your own. Additionally, the Calm app is another very useful tool similar to Headspace. Each app offers a 7-day free trial period so that you can try before you buy. These are only two popular apps; there are many more available, some of which are free to use or have a trial period.
I would love to hear your well-being strategies, whether they are a workplace initiative or something you’ve found that works for you personally. Send me an email with your ideas and experiences (
members@ichpnet.org - Subject: Wellbeing Ideas for Jen.) I would love to hear from you!
References
- Padgett EH, Grantner GR. Pharmacist burnout and stress. US Pharm. 2020:45(5)HS2-HS-10.
- Crank C. Crank's Corner. Positive thinking: an important skill for stressful times. KeePosted. 2020; 46(4):11
- Cain J. Effectiveness of issuing well-being challenges to nudge pharmacy students to adopt well-being protective behaviors. Am J Pharm Educ. 2020;84(8): Article 7875.
 Crank's Corner
Crank's Corner
Get a Hobby. Seriously!
by Christopher W. Crank, PharmD, MS, BCPS; ICHP Executive Vice President
The pandemic has changed many aspects of our lives for the worse. The long-standing mitigation measures have made many people feel isolated, bored, depressed, and stressed. It has not been an easy time to live. However, one positive theme that I have heard many times is that people have used the downtime to develop a new skill or hobby. I know people who have learned new languages, gotten in better shape, or learned crafting hobbies requiring creativity such as woodworking, knitting, or quilting. Hobbies have always been an important part of well-being and resilience efforts; however, they are even more crucial now to well-being.
Hobbies come in all shapes and sizes. They can involve physical activity or mental activity. They can be something in which we are already proficient or something in which we are novices. I know that many may say they do not have time for a hobby. I get it. The pandemic has increased the workload on most people working in healthcare. However, I would argue that this means the need to have a hobby is even greater. Edward Stanley, an English clergyman in the 1800s, recognized the importance of physical activity. He said, “Those who think they have not time for bodily exercise will sooner or later have to find time for illness.” To put it another way, if you do not make time for your physical and mental wellness, you will be forced to make time for your illness. We often make time for the things that are important to us. Sometimes the best way to ensure you make time for your hobby is to schedule it. Schedule the time in your calendar. Sign up for a class where you need to be there to participate at a specific time. Find a hobby that your family can enjoy like cycling so you can exercise, relax, and spend time with your family. In addition, you can join a group or club related to your hobby. These are just some ways that can motivate you to prioritize your hobby.
Hobbies have been associated with benefits such as:
- Improved work performance (engagement, creativity, and problem solving)
- Improved physical health (lower BP, lower cortisol, improved weight)
- Improved mental health and mindfulness
- Lower rates of burnout
- Higher levels of resilience
- Reduced stress
- Better sleep
- Increased social interactions
- Expanded personal network
How do you choose a hobby? A hobby should be something that you enjoy. Even better, it should be something that you can get lost in. For me, these are biking and woodworking. I can always count on these activities to draw me in. I can detach and forget about work and any problems I am having while doing them.
It is also important to assess what your needs are. Do you need more physical activity or mental activity? Do you need a little of both, like I do? There are a multitude of websites that suggest different options. As fun as lounging around watching movies or browsing on your computers may be, most experts recommend that your hobby not involve screentime.
Another option is to think of something that you really enjoyed when you were a kid. I loved biking as a kid, but as I got older, I stopped cycling. Within the last year, I got back into cycling because I needed more exercise and because I remembered how much I love it.
What have you always wanted to try but have not taken the time to learn? Take a class so that you can learn about the hobby you are interested in. The advantage of a class is that it is scheduled time that you can dedicate. Many experts recommend treating hobbies like we do any other goal and scheduling time to work on them.
It is also important to remember that it is okay to start small and try a variety of different hobbies. It may take you a few tries before you find the hobby or hobbies that fit you best.
ICHPeople
Congratulations!
Board of Pharmacy Update
Highlights of the March 2021 Meeting
by Christopher W. Crank, PharmD, MS, BCPS; ICHP Executive Vice President
The March 9th Board of Pharmacy Meeting was held via conference call due to the COVID-19 pandemic. These are the highlights of that meeting.
NABP Updates: No updates
Department Update: Staff member and Board General Counsel Munaza Aman was asked questions related to the continuing education requirements for pharmacy students in Illinois. The primary question revolved around whether pharmacy coursework would be counted toward the continuing education requirements for pharmacy students who are also certified technicians. The Pharmacy Technician Certification Board would require the students to obtain PTCB-approved CE to maintain certification with them. The Department was not able to immediately answer the question of whether the State would accept pharmacy school coursework. The Department plans to provide recommendations on this issue in the near future.
Legislative Update: ICHP Executive Vice President Chris Crank presented the Legislative Update to the Board and reported on several key pieces of proposed legislation.
HB 450: Medicaid-Pharmacy Payments: This bill would require that DHFS and Medicaid MCOs reimburse a pharmacist for the provision of a service or procedure within the scope of the pharmacist's license if the service or procedure: (1) would be covered by the Department or the Medicaid managed care organization if the service were provided by a physician; an advanced practice nurse; or a physician assistant; and (2) is performed by the pharmacist in strict compliance with laws and rules related to the provision of the service or procedure and the pharmacist's license.
Update: Bill did not get out of Committee
HB 2589: Substance Use Disorder-Opioids: This bill would allow for easier distribution of naloxone for patients being discharged from institutions. The proposed legislation would not require a patient-specific label for dispensing the product. Feedback from the Government Affairs Division was provided to the Board. Government Affairs recommended adding language to the bill to require that the naloxone be labeled with instructions for use.
Update: Bill passed in House of Representatives; moved to Senate.
HB 3867: Imported Prescription Drugs: This bill would create the Wholesale Importation of Prescription Drugs Act and would require the Department of Public Health to design an importation program where the State is the licensed wholesaler of imported drugs from licensed, regulated Canadian suppliers.
Update: Bill did not get out of Committee
SB 579: Facility-Provided Medications: This bill would require that an unused portion of a facility-provided medication required for continuing treatment be provided to a patient upon discharge when the facility-provided medication is ordered at least 24 hours in advance for surgical procedures, and that facility-provided medications be labeled in accordance with the Pharmacy Practice Act.
Update: Bill passed in Senate; moved to House of Representatives.
Public Comments: Public comments and questions were primarily in relation to the pharmacy student continuing education requirements outlined previously.
Next Meeting: The next meeting of the Board of Pharmacy is scheduled for May 11th, tentatively potentially in Chicago but most likely via video conference. Interested individuals should monitor the Department’s pharmacy webpage
(www.idfpr.com) for more information. These meetings are open to the public and pharmacists, pharmacy technicians, and pharmacy students are encouraged to attend or listen in.
Government Affairs Report
March 2021 Update
by Christopher W. Crank, PharmD, MS, BCPS; ICHP Executive Vice President
Things are moving again in Springfield, and the Division of Government Affairs is once again reviewing proposed legislation. As mentioned in the March Board of Pharmacy Update, ICHP is currently monitoring more than 100 bills in this spring’s General Assembly session. I have highlighted many of the most important bills in this article. A complete list of the bills being followed by the Government Affairs Division is available online at www.ichpnet.org/pharmacy_practice/advocacy/.
I encourage you to review each one and look to see if your legislators have sponsored any of them. Below are some of the most important bills at this time:
HB 66: Mary Flowers - Amends the Illinois Public Aid Code. Would allow all current participants to enroll in fee-for-service Medicaid as of January 1, 2022. Would also prohibit the state from entering into new contracts with managed care organizations.
Update: Bill did not get out of committee.
HB 76: Mary Flowers - Amends the Pharmacy Practice Act. Would require the following:
- One pharmacy technician on duty whenever the practice of pharmacy is being conducted.
- Pharmacies can fill no more than 10 prescriptions per hour.
- 10 pharmacy technician hours per 100 prescriptions filled.
- 8-hour workday limit
- Pharmacist break periods
The bill would also prohibit advertising or soliciting activities that may jeopardize patient health, safety, or welfare. Whistleblower protections are also included.
Update: Bill did not get out of committee.
HB 99 and HB 119: Numerous sponsors - Creates the Prescription Drug Repository Program Act. Requires the Department of Public Health to, by rule, establish a prescription drug repository program, under which any person may donate a prescription drug or supplies needed to administer a prescription drug for use by an individual who meets eligibility criteria specified by the Department.
Update: HB119 passed in House of Representatives; now in Senate.
HB 135: Michelle Mussman, Deb Conroy, Lindsey LaPointe, and Suzanne Ness - Provides that the definition of "practice of pharmacy" includes the dispensing of hormonal contraceptives pursuant to the standing order under provisions of the Department of Public Health Powers and Duties Law of the Civil Administrative Code of Illinois. Amends the Illinois Public Aid Code. Requires the medical assistance program to cover patient care services provided by a pharmacist for hormonal contraceptives assessment and consultation. Effective January 1, 2022.
Update: Passed in House of Representatives; now in Senate.
HB 309: LaToya Greenwood, Stephanie A. Kifowit, and Barbara Hernandez - Creates the Implicit Bias Training for Health Care Professionals Act. Provides that in order to renew a license as a health care professional in the State, a licensee shall complete an evidence-based implicit bias training, which shall include the promotion of bias-reducing strategies to address how unintended biases regarding race, ethnicity, gender, identity, sexual orientation, socioeconomic status, or other characteristics affect the health care industry.
Update: Did not get out of committee.
HB 450: Deb Conroy, Barbara Hernandez, and Lawrence Walsh, Jr. - Provides that the Department of Healthcare and Family Services and Medicaid managed care organizations may not deny reimbursement to a pharmacist for the provision of a service or procedure within the scope of the pharmacist's license if the service or procedure: (1) would be covered by the Department or the Medicaid managed care organization if the service were provided by a physician; an advanced practice nurse; or a physician assistant; and (2) is performed by the pharmacist in strict compliance with laws and rules related to the provision of the service or procedure and the pharmacist's license.
Update: Did not get out of committee.
HB 585: Dagmara Avelar, Stephanie A. Kifowit, and Barbara Hernandez - Amends the Pharmacy Practice Act. Requires a pharmacy to offer a kiosk to dispose of prescription and over-the-counter medications free of charge.
HB 711, SB 158, and SB 177: Numerous sponsors - Creates the Prior Authorization Reform Act. Provides requirements concerning disclosure and review of prior authorization requirements, denial of claims or coverage by a utilization review organization, and the implementation of prior authorization requirements or restrictions.
HB 711 Update: Passed in House of Representatives; now in Senate.
SB 158 & SB 177 Update: Did not get out of assignments.
HB 2589: Deb Conroy - Amends the Substance Use Disorder Act. Provides that a health care professional or other person acting under the direction of a health care professional may store and, without generating or affixing a patient-specific label, dispense an opioid antagonist to a patient in a hospital, hospital affiliate, or ambulatory treatment center if certain pertinent information is provided to the patient.
Update: Passed in House of Representatives; now in Senate.
HB 2919: Deanne M. Mazzochi - Amends the Illinois Insurance Code. Provides that upon request by a party contracting with a pharmacy benefit manager, the party has an annual right to audit compliance with the terms of the contract by the pharmacy benefit manager, including, but not limited to, full disclosure of any value provided by a pharmaceutical manufacturer to a pharmacy benefit manager or the parent, subsidiary, or affiliate company of a pharmacy benefit manager.
Update: Did not get out of committee.
HB 3244: Natalie A. Manley - Amends the Medical Assistance Article of the Illinois Public Aid Code. Requires all Medicaid managed care organizations to reimburse pharmacy provider dispensing fees and acquisition costs at no less than the amounts established under the fee-for-service program whether the Medicaid managed care organization directly reimburses pharmacy providers or contracts with a pharmacy benefit manager to reimburse pharmacy providers.
Update: Did not get out of committee.
HB 3454: Marcus C. Evans, Jr. - Amends the Illinois Controlled Substances Act. Provides that a prescriber shall offer a prescription for naloxone hydrochloride or another drug approved by the United States Food and Drug Administration for the complete or partial reversal of opioid depression to a patient when one or more of the following conditions are present: (1) the prescription dosage for the patient is 90 or more morphine milligram equivalents of an opioid medication per day; (2) an opioid medication is prescribed concurrently with a prescription for benzodiazepine; (3) the patient presents with an increased risk for overdose, including a patient with a history of overdose, a patient with a history of substance use disorder, or a patient at risk for returning to a high dose of opioid medication to which the patient is no longer tolerant.
Update: Did not get out of committee.
HB 3596: Dagmara Avelar - Amends the Illinois Controlled Substances Act. Provides that, notwithstanding any other provision of law, a prescription for a substance in Schedule II, III, IV, or V must be sent electronically, in accordance with provisions regarding the Prescription Monitoring Program.
Update: Passed in House of Representatives; now in Senate.
HB 3630 and SB 2008: Numerous Sponsors - Amends the Illinois Insurance Code. Provides that if a generic equivalent for a brand-name drug is approved by the federal Food and Drug Administration, plans that provide coverage for prescription drugs through the use of a drug formulary that are amended, delivered, issued, or renewed in the State on or after January 1, 2022 shall comply with specified requirements. Provides that the Department of Insurance may adopt rules to implement provisions concerning notice of change of drug formulary. In provisions concerning a contract between a health insurer and a pharmacy benefit manager, provides that a pharmacy benefit manager must update and publish maximum allowable cost pricing information according to specified requirements, must provide a reasonable administrative appeal procedure to allow pharmacies to challenge maximum allowable costs, and must comply with specified requirements if an appeal is denied. Sets forth provisions concerning pharmacy benefit manager contracts; specified requirements that a pharmacy benefit manager shall comply with; and specified requirements that an auditing entity shall comply with when conducting a pharmacy audit. Provides that a violation of specified provisions is an unfair method of competition and unfair and deceptive act or practice in the business of insurance. Sets forth provisions concerning applicability of the Pharmacy Benefit Managers Article of the Illinois Insurance Code, and provisions concerning fiduciary responsibility of a pharmacy benefit manager. Defines terms. Makes other changes. Amends the Illinois Public Aid Code. Sets forth provisions concerning reimbursement of professional dispensing fees and acquisition costs for pharmacy providers.
HB 3630 Update: Did not get out of committee.
SB 2008 Update: Still in assignments.
HB 3867: Anna Moeller - Creates the Wholesale Importation of Prescription Drugs Act. Requires the Department of Public Health to design an importation program where the State is the licensed wholesaler of imported drugs from licensed, regulated Canadian suppliers.
Update: Did not get out of committee.
SB 142: Laura M. Murphy - Amends the Medical Assistance Article of the Illinois Public Aid Code. Provides that drugs prescribed to residents of the following facilities are not subject to prior approval as a result of the 4-prescription limit: (i) long-term care facilities as defined in the Nursing Home Care Act; (ii) community-integrated living arrangements as defined in the Community-Integrated Living Arrangements Licensure and Certification Act; (iii) supportive living facilities as defined in the Code; (iv) intermediate care facilities for persons with developmental disabilities as defined in the ID/DD Community Care Act; and (v) medically complex for the developmentally disabled facilities as defined in the MC/DD Act.
Update: Third reading deadline 4/30/2021
SB 579: Laura Fine - Amends the University of Illinois Hospital Act, the Ambulatory Surgical Treatment Center Act, the Hospital Licensing Act, and the Pharmacy Practice Act. Requires hospitals and facilities to offer a patient any unused portion of a facility-provided medication upon discharge when it is administered to a patient at the hospital or facility and is required for continuing treatment.
Update: Passed in Senate; Moved to House of Representatives.
SB 1789: Laura M. Murphy - Amends the Illinois Procurement Code. Provides that the Department of Central Management Services, in consultation with the Chief Procurement Officer, shall implement and develop a program to establish a State prescription generic drug label for the purpose of increasing competition in the generic drug market and lowering generic drug prices for all purchasers.
Update: Did not get out of assignments.
New Practitioners Network
Getting Started with #TwitteRx: A Guide to navigating Professional Social Media
by Gabrielle Pierce, PharmD, MBA; PGY1 Specialty Pharmacy Resident; University of Illinois at Chicago
In a time of remote work and social distancing, professional networking has changed drastically. No longer is it the norm to gather for crowded conferences and shake hands with new acquaintances at roundtable sessions. Many pharmacists, pharmacy students, and residents have chosen to connect virtually through professional social media accounts, particularly Twitter. This popular platform allows for sharing advice, publications, words of encouragement, and anecdotes among pharmacists and students across the nation. Below are some tips for getting started and how to make the most out of your #TwitteRx (the chosen trending hashtag for all things pharmacy) experience.
First, there are several things to consider when creating your professional social media account. It is best to use your full name so that it is easy for others to recognize you from your publications and presentations. Be sure to choose a username that is easy to share with others; you get bonus points if you are clever enough to develop a pharmacy-related pun to incorporate. Also, use a profile photo that clearly shows your face. This does not need to be a professional headshot, just a close-up photo that is recognizable as you! These pieces serve as the backbone of your personal brand.
Next, the challenge becomes deciding who you would like to connect with or “follow.” A good place to start is following colleagues at your institution or former pharmacy school classmates who may be active on Twitter. Following professional organizations such as ICHP (@ICHPnet), ASHP (@ASHPOfficial), and others will also allow you to stay up to speed with upcoming events and connect with peers. Another great way to find fellow pharmacists is to use the search function and type in the hashtag commonly used by the pharmacy Twitter community, #TwitteRx. This should bring up individuals who have this hashtag in their profile and recent tweets shared on the platform. I would also encourage you to follow other healthcare professionals; social media is a great way to build relationships and share ideas with trainees and practitioners in all aspects and specialties of healthcare. Building a network comprised of individuals at every level of training - from first-year students to attending clinicians at major health systems, is an excellent way to build a balanced feed with many perspectives.
As a bonus tip, several other hashtags can help identify individuals and content that may be of interest based on your scope. Often, #PharmRes is used as a hashtag for tweets about pharmacy residency training, recruiting, or resident development. #PharmEd is commonly used among pharmacy educators to share ideas related to academia. These hashtags allow users to tailor their feed based on interest areas.
Sharing relevant and engaging content is another aspect of social media that often can be difficult, but there are several easy ways to develop ideas. If you learn something new throughout your day – share it! You may see people sharing “one thing I learned today” and using the hashtag #OTILT to educate followers. Posting clinical pearls learned via real-world experience is invaluable and encourages ad hoc continuing education throughout the platform. Similarly, if you read a journal article that you find interesting, share a link to the article with your thoughts and takeaways. In this case, it is even better to tag the social media accounts of any of the authors in your post. Do not be afraid to retweet (which is Twitter’s version of sharing another person’s post) any content you find interesting and include your thoughts. Engagement with others is an effective strategy for building your social media network. Summarizing or organizing your ideas into a thread (i.e., multi-tweet post) or, even better, creating an infographic (i.e., downloadable visual file) is an excellent way of teaching others and expanding your influence.
Whether virtual or in-person, conferences or summits provide valuable opportunities to show off your savvy social media and networking skills. Most conferences will have a hashtag that can link users and content related to the event. Sharing photos, weblinks, and impressions about the presentations and sessions that you attend is a great way to interface with others who may be attending the same event as well as provide insight for those unable to attend.
Finally, be sure that you are using Twitter in a way that allows you to build connections with others. A great way to do this is through peer recognition and encouragement. If a colleague posts about a clinical success story, academic accomplishment, or even just a fun birthday, respond and offer positive words of congratulations. If you come across an article or presentation given by someone you have followed on Twitter, post about it and acknowledge their excellent work. This is a great way to pay it forward and offer support to others in the profession. Often, pharmacists will crowdsource for input related to clinical conundrums, professional development, or personal struggles. It is also a great space for sharing photos of your favorite pets or future vacation spots to break up the lulls in the day. If you find yourself overwhelmed by Twitter or may be hesitant to take the plunge, you can always “like” the posts of other pharmacists as an initial step to becoming more comfortable with the platform; this is a great way to start engaging with others if you are not yet ready to start posting any content yourself.
Though social media may not be the traditional professional networking method, many meaningful relationships can be built through its use. Many pharmacists use social media to share job openings at their institutions, volunteer experiences in their communities, new clinical literature, and opportunities for collaborative projects. Don’t miss out on some of these opportunities by turning your back on social media. Through positive engagement and a willingness to learn from others, #TwitteRx can be a great way to improve your practice as a pharmacist and build your network from the comfort of your own home.
References:
Dixon D, Reed B. To tweet or not to tweet? A primer on social media for pharmacists. J Am Coll Clin Pharm. May 2019. Doi: 10.1002/jac5.1120.
PEARLS: Public Education & Awareness Outreach Publication Subcommittee
Expanding Pharmacy's Reach One Tweet At a Time!
by Andrew Merker, PharmD, BCPS, BCIDP, AAHIVP; Assistant Professor, Midwestern University College of Pharmacy - Downers Grove; NISHP President
Importance of a Pharmacy Social Media Presence
Social media platforms (SMP), such as Twitter, Facebook, Instagram, and LinkedIn, have shown to be powerful tools for communicating and sharing information. Pharmacists have a unique position to disseminate essential and influential information to patients as well as friends and family.
Utilizing social media in an informative and professional manner can increase public awareness regarding the pharmacist’s role in the healthcare setting. Additionally, a trusted pharmacist who shares or disseminates useful and accurate healthcare information through social media can educate the public in an ever-changing healthcare world.
Potential Applications for Social Media Platforms
- Marketing for a pharmacy
- Disseminating vital health care information
- Rebuttal of inaccurate health care information
- Developing and maintaining patient-pharmacist and provider-pharmacist relationships
- Developing and maintaining relationships with pharmacist colleagues
- Advocating for disease states, patient care, and the pharmacy profession
Benefits and Potential Consequences of a Social Media Presence
Utilizing and communicating through SMP can have several potential benefits. Friends, family, and the general public can receive greater pharmacist accessibility from a trusted source. With this accessibility, it can help empower social media users regarding disease states or their medications. Pharmacists can impact conversations regarding challenging healthcare-related issues and provide social media users with accurate and vital information. The dissemination of such information can increase the visibility of pharmacists within the healthcare field to the public and spread awareness of the role pharmacists play in patient care.
Although SMP can be a convenient method for patient, pharmacy, and healthcare advocacy, it is crucial to understand the potential limitations and when a patient or potential social media audience would be best served through other means. Maintaining patient privacy is a must to avoid potential HIPAA violations. Even when using a personal social media account, it is important to manage the pharmacist’s persona on the SMP professionally as inappropriate posts can harm the individual pharmacist’s and the pharmacy profession’s reputation.
Recommendations for Utilizing Social Media Platforms
Direct Patient Care - Be cautious when providing individualized patient recommendations for care over SMP. There are several concerns about providing such recommendations that include maintaining patient confidentiality, an incomplete understanding and knowledge of the patient's medical history, and the obligations/liabilities associated with developing a pharmacist-patient relationship.
Maintain Professionalism and Reputation - Regardless of healthcare or non-healthcare-related posts, it is crucial to maintain the pharmacy profession's high professional standards. SMP should not be used to complain about patient encounters as this does not advance the pharmacy profession or protect patients' dignity. Posting inappropriate or unprofessional content, regardless of who the posts are directed to or if they include non-healthcare content, can harm an individual pharmacist’s reputation and impair the public’s trust in the profession. When discussing information with SMP users, it is essential to maintain civility and avoid disparaging remarks.
Ensure Privacy - Sharing healthcare information, including protected health information (such as name, email address, pictures, addresses), could be a potential HIPAA violation that may result in civil or criminal offenses. Avoid discussing patient-specific information in a public or non-encrypted online environment. Discussing patient information in these settings has several patient identifiers attached to it. If individuals ask to discuss personal data, it may be best to discuss it personally or over the phone in a private setting.
Disseminate Accurate Information - Healthcare information distributed through SMP should be in accordance with the professional standards of pharmacy practice and originate from well trusted, reputable organizations. Providing inaccurate information that does not comply with pharmacy practice standards can result in patient harm, decreased trust in the individual pharmacist and the pharmacy profession. Before posting, the pharmacist should be well versed in the topic subject.
Conflict of Interest - Before posting statements involving the promotion of a business or potential financial benefits for the pharmacist posting, declaring a potential conflict of interest is vital to allow the patient/public to understand possible user bias.
Review Institutional Policies - Employers or institutions may have policies in place that involve employees posting information or comments on SMP relating to professional or healthcare-related activities on personal SMP. Before using SMP in a healthcare-related manner, review institutional policies.
Summary
Pharmacists are consistently one of the most trusted professions by the public. Social media platforms allow pharmacist users to quickly and easily share their knowledge and expertise with a large number of people. The potential benefits are limitless, and pharmacists and pharmacy organizations should promote SMP use in this setting. When maintaining an SMP persona, it is important to remember that it should be done professionally, regardless of how it is being used. When providing education through online sources, pharmacists should employ the high standard of pharmacy practice to ensure information is accurate and trusted to advance the interests of the public and the pharmacy profession.
If you’re new to posting pharmacy and healthcare-related topics on social media or don’t know what to post, make sure to follow ICHP on Facebook and Twitter. These social media feeds will be posting information regarding the pharmacist's role in health care that can be used to start conversations on important topics, such as vaccinations, opioid antidotes, and monitoring blood pressure. Feel free to share these posts on your social media feeds and help your friends and family stay informed on the services pharmacists can provide!
ICHP Leadership Spotlight
Meet Vera Kalin, CPhT
What is your leadership position within ICHP?
Technician Representative for NISHP. I represent Illinois hospital technicians. I relay issues that are discussed in our ICHP and NISHP meetings with my fellow technicians. I also give feedback on the type of topics technicians would be interested in hearing about.
Describe your practice site?
I have been at Rush since 1989. For many years I was the primary IV room technician. I trained new technicians and pharmacy students. I still enjoy sharing my knowledge and experience. Now I work in a variety of different roles and different clinics, but I still enjoy the IV area.
How did you select pharmacy as a career?
I feel pharmacy selected me. The hospital I was working at as an LPN was phasing out LPNs. My supervisor suggested working in the pharmacy as a pharmacy technician. I had never even heard of such a thing. I decided to give it a try. After a year, the hospital I was working at closed and I moved on to another hospital, where I continued to work as a technician. I was, and still am, amazed by all the behind-the-scenes work and knowledge involved. I feel I hit the technician lotto. I joined the world of pharmacy and never looked back.
What did you learn at an ICHP event that you implemented in to your practice?
There is a lot of information out there. The majority of it is about new drugs that will soon be available, such as the COVID-19 vaccines. We started talking about the vaccines when they were in their early stages. It is so exciting and I felt privileged to be so informed. I am so fortunate. I often share the new information I learn at ICHP with my coworkers.
What makes ICHP great?
All the knowledge that such seasoned pharmacists bring to the table. Had I not joined ICHP, I would have missed out on a once in a lifetime opportunity to learn from the best.
What initially motivated you to get involved in ICHP?
I finally took the plunge and actually signed up and joined ICHP when a former co-worker and technician brought me the registration form and said “just sign”. It was that easy. She was also a NISHP Technician Representative at the time.
Is there an individual you admire or a mentor that has influenced your career?
I would say it is the students. When I started at Rush I was younger than the students. I hung out with them and they showed me a lot and discussed many aspects of things that they were learning. Students were the ones who told me about ICHP and always encouraged me to join. I am so grateful I took their advice. I also enjoy seeing and catching up with so many amazing, former co-workers who I used to work with at Rush. They are now doing even more incredible work within ICHP. It is such an honor to have worked with them and to continue to work with them through ICHP.
What advice would you give to student pharmacists?
Please share your knowledge and your love of pharmacy with technicians.
What's an interesting fact about you?
I speak several languages. I enjoy speaking them, especially at our live meetings. I am fluent in Ukraine and speak a few others.
What 3 adjectives would people use to describe you?
Best one-liners
Is that singing?
Can’t stop dancing.
ICHP Leadership Spotlight
Meet Radhika S. Polisetty, PharmD, BCIDP, BCPS AQ-ID, AAHIVP
What is your leadership position within ICHP?
I am currently the Secretary of NISHP (Northern Illinois Society of Health-System Pharmacists).
Describe your practice site.
I work as an Associate Professor of Pharmacy Practice at Midwestern University College of Pharmacy in Downers Grove. I also practice as an Infectious Diseases/Antimicrobial Stewardship Pharmacist at Northwestern Medicine Central DuPage Hospital in Winfield, IL.
Tell us about a time when you made a difference at work.
At the start of the COVID pandemic, as an Infectious Diseases Specialist, I was tasked with coming up with a COVID treatment protocol for our institution and also enrolling our hospital as a site for clinical trials and expanded access protocols for medications such as remdesivir (which has since received FDA approval). I worked closely with our research team to help ensure our patients had access to the upcoming therapeutic options as they became available.
What pharmacy-related issues keep you up at night?
I think as an inpatient acute care pharmacist, the medication shortages are really hurting our patients. It is a complex issue with no easy solutions, so it does keep me up at night. This issue also hits home harder for me as an ID specialist because we do not have many therapeutic options left for patients with multidrug-resistant organisms.
What makes ICHP great?
I think what makes ICHP great is that they put patient care first and provide pharmacists and technicians from various specialties the tools they need to succeed at their jobs and grow in their careers. I am also very impressed by the resources that they provide students and residents in terms of medical education as well as leadership opportunities.
What initially motivated you to get involved in ICHP?
When I first moved to IL and started my position as a faculty member at Midwestern University, I had the opportunity to work with some of my colleagues to provide an ICHP educational session. It was a very rewarding experience and I continued to participate in future educational events as a speaker and as a participant. I have learned so much by networking with my peers and hearing what others are doing at their respective institutions.
is there an individual that you admire or look up to, or a mentor that has influenced your career?
I am so grateful to have a several faculty mentors and friends who have provided me with guidance, support and advice throughout my career. I would not have been able to establish my service at my clinical site or succeed as an educator without their help. I strive to pay it forward and try to be a resource for my students, trainees and junior faculty members.
What advice would you give to student pharmacists?
Don’t be afraid to pursue your ideas or seek opportunities outside your comfort zone. You will always find help if you seek it. Don’t let pre-conceived notions and old biases keep you from achieving bold new things.
What are your special interests or hobbies outside of work?
Outside of work I love to spend time with my family, travel and listen to music.
Where is your favorite place to vacation?
Oh that is a tough one. I love to travel and it is hard for me to pick a favorite! Will go with Europe because I love the scenic views, art, history and food there.
Professional Affairs
Safety Skills for Everyday Interactions
by Paul Fina, PharmD, BCACP, BCPS; Clinical Assistant Professor, Chicago State University Medication Safety Officer, Cook County Health and Hospital System, John H. Stroger Hospital, Chicago, IL
You just arrived for the start of your shift at the inpatient pharmacy when you answer the phone for the first time for the day. On the other end of the call is a very upset nurse, calling about a patient’s missing antibiotic dose. She berates the pharmacy department for a lack of competency during the call and you start to get upset as well because of the interaction. Or, consider another scenario. Today is the first day you are participating as a vaccinator in a COVID-19 vaccine clinic at your hospital. The institution’s vaccinator training emphasized the importance of reviewing an identification prior to administering the vaccine. Your first patient for the day unfortunately arrived without identification and was extremely angry when you turned them away. The challenging part of the interaction was that this patient is also a physician at your hospital!
Healthcare is a high stakes environment by its very nature; the health and well-being of our patients hang in the balance with every interaction. This can create a highly emotional environment due to the stakes - healthcare providers understand the importance of their actions and decisions and as a result, want to ensure the best care possible for their patients. However, healthcare providers have different backgrounds and training, which inevitably results in different opinions on the best course of action. The outcome of this environment is a major safety challenge, as unintended task-conflict can exist among providers, patients, and service lines. Conflicts such as these can become relationship-conflict, causing stakeholders to withdraw from conversations or lash out at co-workers. Ultimately, the team suffers as “being on the same page” becomes harder without an open dialogue. This may not be your experience and I’m not suggesting that conflict cannot be productive. In fact I suggest the opposite – that how conflict is managed can affect relationships among all stakeholders as well as institutional culture. Here I present several free and low-cost resources available to help navigate and overcome conflict in the healthcare workspace.
Crucial Conversations is a book with years of research behind it that I highly recommend for having “safe” high stakes conversations in healthcare.1 According to the book, crucial conversations are discussions when stakes are high, emotions are strong, or participants have opposing views. Therefore, many conversations in healthcare could be considered crucial conversations. Knowing this definition, recall the last time (it doesn’t have to be work related) that you had a crucial conversation when you were emotional. How did you react? Did you quietly seethe in your rage, or did you go on the attack to prove your point? Either reaction is counter-productive to finding an outcome amenable to all parties. This book presents tools and philosophies for ensuring a more productive crucial conversation. I encourage you to read the book on your own, but here are three key processes/philosophies I want to highlight:
- Focus on yourself first. You are the only person that you can fully control. How you present yourself, approach the conversation, and react to the other party’s reaction to conflict are the only things you can control. Other parties in the discussion may not have the reaction you wish for, but that is okay. Focus on yourself.
- Make conversations safe. Dialogue can only happen when people contribute to the conversation and that can only happen when people feel safe to express their concerns and ideas. Restore safety when you sense the conversation taking a turn for the worse. Safety can be restored by finding mutual purpose, ensuring mutual respect, and apologizing when appropriate.
- Use STATE.
- Share your facts – Leading with facts ensures all parties understands the origin of your view. Facts are not controversial or insulting, and they can be persuasive.
- Tell your story – This can be a bit scary, but is also the moment when you present your conclusion from the facts you have gathered.
- Ask for others' paths – Gain an understanding of what others' viewpoints are.
- Talk tentatively – This means not presenting your story as a hard conclusion.
- Encourage testing – Invite opposing views, it’s important to hear everything, identify controversy, and build consensus.
The second resource you should consider exploring is the Team Strategies and Tools to Enhance Performance and Patient Safety (TeamSTEPPS) program.2 It is an evidence-based system developed by the Agency for Healthcare Research and Quality (AHRQ) and Department of Defense (DoD) to optimize patient care and teamwork among healthcare professionals. The resource is a 7-course core module that can be taken without additional guidance (ie. classroom slides are available online along with a pocket guide). However, if a more formal roll-out is desired, an instructor’s guide, implementation guide, and practice scenarios are also available. Additionally, there are TeamSTEPPS practice-focused courses that may be of better use to you and include long-term care, rapid response, and office-based care. The most streamlined version of the TeamSTEPPS content is their Essentials course.3
There is A LOT to the TeamSTEPPS program; some concepts are briefly described here. Four teachable/learnable skills are the foundation for team-based care – communication, leadership, situation monitoring, and mutual support.2 The program emphasizes several high-yield safety communication strategies. These include Situation-Background-Assessment-Recommendation/Request (SBAR) reports which convey critical information in a structured way; call-outs which are announcements that inform all team members simultaneously; check-backs which close the communication loop by providing feedback on the information received; and hand-offs which transfer information and responsibility. TeamSTEPPS also identifies three “CUS” words/phrases, which should be used when in a safety situation – “I am CONCERNED,” “I am UNCOMFORTABLE,” and “this is a SAFETY issue.” The program also recommends using briefs, huddles, and debriefs to ensure mutual understanding of the plan, responsibilities, and expected outcomes. Lastly, a high-functioning team has mutual support, which is a climate where assistance is actively sought and offered. A provider can implement TeamSTEPPS practices without an institutional roll-out, so please consider utilizing these strategies.
This short commentary cannot replace any kind of safety related training. However, some of the presented processes can be immediately implemented. Self-exploration, reflection, self-awareness, and coordinated institutional implementation are necessary to cultivate a safety culture at your workplace. Overall, there are many available safety systems and programs, and there is significant overlap among them. The goal is the same for each, so determine which is best for you and work towards safety every day at work. Safety starts with you.
References
- Patterson K, Grenny J, McMillan R, Switzler A. Crucial conversations: Tools for talking when stakes are high. New York, NY: McGraw-Hill; 2012.
- Curriculum Materials. Content last reviewed October 2019. Agency for Healthcare Research and Quality, Rockville, MD. https://www.ahrq.gov/teamstepps/curriculum-materials.html.
- Essentials Instructional Module and Course Slides. Content last reviewed March 2014. Agency for Healthcare Research and Quality, Rockville, MD. https://www.ahrq.gov/teamstepps/instructor/essentials/index.html.
Educational Affairs
To Reduce or Not to Reduce? Insulin Dose Adjustments Upon Starting GLP-1 Receptor Agonists
by Abigail T. Elmes, PharmD, BCPS Research Fellow in Academia and Family Medicine; University of Illinois at Chicago College of Pharmacy - Chicago, IL; Daphne E. Smith Marsh, PharmD, BC-ADM, CDCES Clinical Assistant Professor/Clinical Pharmacist; Dept. of Pharmacy Practice College of Pharmacy/Mile Square Health Center, UI Health - Chicago, IL; Brianna M. McQuade, PharmD, BCACP, MHPE Clinical Assistant Professor; University of Illinois at Chicago College of Pharmacy, Mile Square Center - Chicago, IL; Jennie B. Jarrett, PharmD, BCPS, MMedEd, FCCP Assistant Professor; Clinical Pharmacist, Family Medicine, University of Illinois at Chicago College of Pharmacy - Chicago, IL
The development of glucagon-like peptide-1 receptor agonists (GLP-1RAs), such as exenatide, liraglutide, dulaglutide, lixisenatide, and semaglutide, led to major significant advances in type 2 diabetes (T2DM) management. GLP-1RAs improve insulin secretion in a glucose-dependent manner, slow gastric emptying, increase satiety, increase glucose uptake by the muscles, decrease gluconeogenesis in the liver, and reduce postprandial glucagon secretion.1 These agents offer many advantages given their significant reduction of hemoglobin A1c (A1C)2, promotion of weight loss3, reduced risk of hypoglycemia, and reduced major adverse cardiovascular outcomes4–6 and reduced progression of nephropathy.7
The American Diabetes Association recommends initiating GLP-1RAs in patients with T2DM after implementing lifestyle modifications and metformin therapy if promoting weight loss, minimizing weight gain, or decreasing hypoglycemia is desired.8 GLP-1RAs with proven cardiovascular disease benefits (dulaglutide, liraglutide, or semaglutide) are recommended in patients with atherosclerotic cardiovascular disease (ASCVD) or chronic kidney disease without albuminuria. Additionally, GLP-1RAs are the preferred injectable agent over insulin for patients on oral therapy needing intensification.8 Insulin should be prioritized over a GLP-1RA in patients with A1C >10% or blood glucose levels >300 mg/dL or weight loss AND symptoms of hyperglycemia.8
For patients on basal insulin, GLP-1RAs are the preferred addition over prandial insulin due to clearer dose titration and patient education and as well as a reduced risk of hypoglycemia and fluctuations in blood glucose.8,9 Combination products like Xultophy™ (insulin degludec/liraglutide) and Soliqua™ (insulin glargine/lixisenatide) offer the advantage of reduced administrations by combining basal insulin and a GLP-1RA in a single injection.10
Due to their extended time on the receptor, longer-acting GLP-1RAs have a greater effect on FBG and PPG compared to shorter-acting agents, which have targeted effects on PPG (Table 1).9 Some clinical trials have described anticipatory reductions in basal insulin dose by 10-20% when initiating a GLP-1RA in more adequately controlled patients (A1C <8%). These adjustments are based on clinical knowledge and are not consistent or well-studied.9 Table 2 outlines clinical trials and recommendations for insulin adjustments with GLP-1RAs. However, best practices are needed for insulin adjustments when initiating a GLP-1RA.
.jpg)
.jpg)
In 2015, researchers at the Oxford Centre for Diabetes Endocrinology and Metabolism released recommendations for a 10% reduction in basal insulin and 30-40% reduction in prandial insulin upon addition of a GLP-1RA.11 Few studies specifically evaluating insulin dose adjustments in GLP-1RA initiation have been published since this recommendation. A randomized, double-blind, placebo-controlled trial in Sweden evaluated the addition of once-daily liraglutide to patients inadequately controlled on basal-bolus insulin therapy.12 Because patients had suboptimal glycemic control at baseline (A1C ≥7.5%), insulin doses were not preemptively reduced. If FBG or pre-prandial glucose levels were normal or close to normal for two consecutive days, then dose reductions were considered. After 24 weeks, reductions were found between liraglutide versus placebo for A1C (-1.13 [95% CI -1.45 to -0.81]), body weight (-3.81 kg [95% CI -4.87 to -2.76]), and total daily insulin dose (-15.8 units [95% CI -23.1 to -8.5]). There was no difference in hypoglycemia between the groups.12
A 26-week, randomized, open-label, active-control, multicenter, treat-to-target study compared patients with T2DM with an A1C 7.0 to 9.5% with or without metformin on a basal-bolus insulin regimen (<140 units/day and at least 3 three injections/day) versus the addition of albiglutide and reduction of prandial insulin. All patients were standardized on once-daily insulin glargine and three times-daily insulin lispro before randomization. In the albiglutide and insulin glargine (AIG) group, the insulin lispro dose was reduced by 50% and subsequently discontinued at week 4 for the remainder of the treatment period. After week 8, insulin lispro was reintroduced in patients with average PPG >180 mg/dL. The insulin glargine-lispro (IGL) arm served as the active control, and insulin lispro dose adjustments were made following an algorithm. The AIG group was non-inferior to the IGL group for change in A1C from baseline (0.06% [95% CI -0.05 to 0.17]). The proportion of patients achieving A1C <7% was similar between groups (OR 1.0 [95% CI 0.7-1.3]). In the AIG group, 72% of patients either did not require insulin lispro reintroduction or decreased the insulin lispro without increasing A1C, and 54% completely replaced insulin lispro with albiglutide at the study conclusion. There were no differences in baseline characteristics between the patients in the AIG group who did or did not require reintroduction of insulin lispro.
Reductions were found between AIG versus IGL for average weekly injections (-16.0 ± 7.9), body weight (-4.4 kg [95% CI -4.9 to -3.8]), total daily insulin dose (-61.8 units [95% CI -65.9 to -57.8]), and hypoglycemic rate (OR 0.43 [95% CI .031-0.60]). Of note, albiglutide was removed from the U.S. market in 2017 for economic reasons unrelated to safety or efficacy.13,14 The study showed a similar mean insulin glargine dose between groups with a lower FBG in the AIG group, emphasizing the impact of long-acting GLP-1RAs on both FBG and PPG.15 Therefore, basal insulin dose reductions may be more appropriate with long-acting agents versus short-acting agents. Table 1 outlines recommendations for short- and long-acting GLP-1RAs initiation with various insulin regimens.
In diabetes management, a patient-centered approach and strong clinical judgment are imperative. For example, in patients at higher risk of hypoglycemia, (longer duration of diabetes, concomitant secretagogues, erratic eating patterns, and kidney disease), more substantial insulin dose reductions may be appropriate.16 Consider the patient case outlined in Figure 1. GLP-1RA initiation is appropriate in this patient, given their elevated A1C, obesity, and ASCVD. Because the A1C is relatively close to the patient’s goal, a 10-20% reduction in basal insulin dose and a 30-50% reduction in prandial insulin dose is appropriate upon starting a long-acting GLP-1RA. If the patient were less adequately controlled, less aggressive insulin dose adjustments could be considered, if at all. Close monitoring of FBG, PPG, and signs/symptoms of hypo- and hyperglycemia is warranted in patients on insulin starting any GLP-1RA.
References:
- Collins L, Costello RA. Glucagon-like peptide-1 receptor agonists. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2020. http://www.ncbi.nlm.nih.gov/books/NBK551568/. Accessed November 18, 2020.
- Htike ZZ, Zaccardi F, Papamargaritis D, Webb DR, Khunti K, Davies MJ. Efficacy and safety of glucagon-like peptide-1 receptor agonists in type 2 diabetes: A systematic review and mixed-treatment comparison analysis. Diabetes Obes Metab. 2017;19(4):524-536. doi:10.1111/dom.12849
- Shyangdan DS, Royle P, Clar C, Sharma P, Waugh N, Snaith A. Glucagon-like peptide analogues for type 2 diabetes mellitus. Cochrane Database Syst Rev. 2011;(10):CD006423. doi:10.1002/14651858.CD006423.pub2
- Varin EM, McLean BA, Lovshin JA. Glucagon-like peptide-1 receptor agonists in adult patients with type 2 diabetes: review of cardiovascular outcome trials. Can J Diabetes. 2020;44(1):68-77. doi:10.1016/j.jcjd.2019.08.011
- Marso SP, Daniels GH, Brown-Frandsen K, et al. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2016;375(4):311-322. doi:10.1056/NEJMoa1603827
- Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2016;375(19):1834-1844. doi:10.1056/NEJMoa1607141
- Dicembrini I, Nreu B, Scatena A, et al. Microvascular effects of glucagon-like peptide-1 receptor agonists in type 2 diabetes: a meta-analysis of randomized controlled trials. Acta Diabetol. 2017;54(10):933-941. doi:10.1007/s00592-017-1031-9
- American Diabetes Association. Pharmacologic approaches to glycemic treatment: standards of medical care in diabetes—2021. Diabetes Care. 2021;44(Supplement 1):S111-S124. doi:10.2337/dc21-S009
- Anderson SL, Trujillo JM. Basal insulin use with GLP-1 receptor agonists. Diabetes Spectr. 2016;29(3):152-160. doi:10.2337/diaspect.29.3.152
- Nuffer W, Guesnier A, Trujillo JM. A review of the new GLP-1 receptor agonist/basal insulin fixed-ratio combination products. Ther Adv Endocrinol Metab. 2018;9(3):69. doi:10.1177/2042018817752315
- Artigas CF, Stokes V, Tan GD, Theodorakis MJ. Insulin dose adjustments with add-on glucagon-like peptide-1 receptor (GLP-1R) agonists in clinical practice. Expert Opin Pharmacother. 2015;16(10):1417-1421. doi:10.1517/14656566.2015.1052740
- Lind M, Hirsch IB, Tuomilehto J, et al. Liraglutide in people treated for type 2 diabetes with multiple daily insulin injections: randomised clinical trial (MDI Liraglutide trial). BMJ. 2015;351. doi:10.1136/bmj.h5364
- Walmsley E. GlaxoSmithKline investor event. Presented at the: GSK Investor Event; July 26, 2017; London, UK.
- Rosenstock J, Nino A, Soffer J, et al. Impact of a weekly glucagon-like peptide 1 receptor agonist, albiglutide, on glycemic control and on reducing prandial insulin use in type 2 diabetes inadequately controlled on multiple insulin therapy: a randomized trial. Diabetes Care. 2020;43(10):2509-2518. doi:10.2337/dc19-2316
- Bolli GB, Porcellati F, Meier JJ. Switching from insulin bolus treatment to GLP-1 RAs added to continued basal insulin in people with type 2 diabetes on basal-bolus insulin. Diabetes Care. 2020;43(10):2333-2335. doi:10.2337/dci20-0038
- Silbert R, Salcido-Montenegro A, Rodriguez-Gutierrez R, Katabi A, McCoy RG. Hypoglycemia among patients with type 2 diabetes: epidemiology, risk factors, and prevention strategies. Curr Diab Rep. 2018;18(8):53. doi:10.1007/s11892-018-1018-0
- Victoza (liraglutide) prescribing information. Plainsboro, NJ: Novo Nordisk Inc; 2020 Aug.
- Byetta (exenatide) prescribing information. Wilmington, DE: AstraZeneca Pharmaceuticals LP; 2020 Feb.
- Bydureon (exenatide extended-release) prescribing information. Wilmington, DE: AstraZeneca Pharmaceuticals LP; 2020 Feb.
- Trulicity (dulaglutide) prescribing information. Indianapolis, IN: Lilly USA, LLC; 2020 Sept.
- Ozempic (semaglutide injection) prescribing information. Plainsboro, NJ: Novo Nordisk Inc; 2020 Sept.
- Rybelsus (semaglutide tablets) prescribing information. Plainsboro, NJ: Novo Nordisk Inc; 2020 Jan.
- Adlyxin (lixisenatide) prescribing information. Bridgewater, NJ: Sanofi-Aventis U.S. LLC; 2019 Jan.
- Tanzeum (albiglutide) prescribing information. Research Triangle Park, NC: GlaxoSmithKline LLC; 2017 Sept.
- Xultophy (insulin degludec and liraglutide) prescribing information. Plainsboro, NJ: Novo Nordisk Inc; 2019 Nov.
- Soliqua (insulin glargine and lixisenatide) prescribing information. Bridgewater, NJ: Sanofi-Aventis U.S. LLC; 2019 Nov.
- Davies MJ, Bain SC, Atkin SL, et al. Efficacy and safety of liraglutide versus placebo as add-on to glucose-lowering therapy in patients with type 2 diabetes and moderate renal impairment (LIRA-RENAL): a randomized clinical trial. Diabetes Care. 2016;39(2):222-230. doi:10.2337/dc14-2883
- Buse JB, Bergenstal RM, Glass LC, et al. Use of twice-daily exenatide in basal insulin–treated patients with type 2 diabetes. Ann Intern Med. 2011;154(2):103-112. doi:10.7326/0003-4819-154-2-201101180-00300
- Diamant M, Nauck MA, Shaginian R, et al. Glucagon-like peptide 1 receptor agonist or bolus insulin with optimized basal insulin in type 2 diabetes. Diabetes Care. 2014;37(10):2763-2773. doi:10.2337/dc14-0876
- Guja C, Frías JP, Somogyi A, et al. Effect of exenatide QW or placebo, both added to titrated insulin glargine, in uncontrolled type 2 diabetes: The DURATION-7 randomized study. Diabetes Obes Metab. 2018;20(7):1602-1614. doi:10.1111/dom.13266
- Pozzilli P, Norwood P, Jódar E, et al. Placebo-controlled, randomized trial of the addition of once-weekly glucagon-like peptide-1 receptor agonist dulaglutide to titrated daily insulin glargine in patients with type 2 diabetes (AWARD-9). Diabetes Obes Metab. 2017;19(7):1024-1031. doi:10.1111/dom.12937
- Rodbard HW, Lingvay I, Reed J, et al. Semaglutide added to basal insulin in type 2 diabetes (SUSTAIN 5): a randomized, controlled trial. J Clin Endocrinol Metab. 2018;103(6):2291-2301. doi:10.1210/jc.2018-00070
- Mosenzon O, Blicher TM, Rosenlund S, et al. Efficacy and safety of oral semaglutide in patients with type 2 diabetes and moderate renal impairment (PIONEER 5): a placebo-controlled, randomised, phase 3a trial. Lancet Diabetes Endocrinol. 2019;7(7):515-527. doi:10.1016/S2213-8587(19)30192-5
- Zinman B, Aroda VR, Buse JB, et al. Efficacy, safety, and tolerability of oral semaglutide versus placebo added to insulin with or without metformin in patients with type 2 diabetes: the PIONEER 8 trial. Diabetes Care. 2019;42(12):2262-2271. doi:10.2337/dc19-0898
- Riddle MC, Aronson R, Home P, et al. Adding once-daily lixisenatide for type 2 diabetes inadequately controlled by established basal insulin: a 24-week, randomized, placebo-controlled comparison (GetGoal-L). Diabetes Care. 2013;36(9):2489-2496. doi:10.2337/dc12-2454
- Seino Y, Min KW, Niemoeller E, Takami A, EFC10887 GETGOAL-L Asia Study Investigators. Randomized, double-blind, placebo-controlled trial of the once-daily GLP-1 receptor agonist lixisenatide in Asian patients with type 2 diabetes insufficiently controlled on basal insulin with or without a sulfonylurea (GetGoal-L-Asia). Diabetes Obes Metab. 2012;14(10):910-917. doi:10.1111/j.1463-1326.2012.01618.x
- Riddle MC, Forst T, Aronson R, et al. Adding once-daily lixisenatide for type 2 diabetes inadequately controlled with newly initiated and continuously titrated basal insulin glargine: a 24-week, randomized, placebo-controlled study (GetGoal-Duo 1). Diabetes Care. 2013;36(9):2497-2503. doi:10.2337/dc12-2462
- Rosenstock J, Fonseca VA, Gross JL, et al. Advancing basal insulin replacement in type 2 diabetes inadequately controlled with insulin glargine plus oral agents: a comparison of adding albiglutide, a weekly GLP-1 receptor agonist, versus thrice-daily prandial insulin lispro. Diabetes Care. 2014;37(8):2317-2325. doi:10.2337/dc14-0001
Educational Affairs
Baricitinib EUA Shakes Up COVID-19 Therapy: What You Need To Know
by Dan Majerczyk, PharmD, BCPS, BC-ADM, CACP; Assistant Professor of Clinical Sciences - Roosevelt University, College of Science, Health and Pharmacy - Schaumburg, IL; Clinical Pharmacy Specialist - Loyola Medicine -MacNeal Family Medicine Residency Program - Berwyn, IL; Janki Vyas, PharmD Candidate 2022 Student - Southern Illinois University Edwardsville School of Pharmacy - Edwardsville, IL; Part-time Pharmacy Intern - South City Hospital/CVS Pharmacy - St. Louis, MO; Ashley Stefanski, PharmD Clinical Instructor, Academic Fellow Roosevelt University, College of Science, Health and Pharmacy - Schaumburg, IL
Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) contributing to coronavirus disease 2019 (COVID-19), continues to plague the United States (U.S.) and the world. With a reported 30 million confirmed cases and over 500,000 deaths in the U.S. alone, the need for lifesaving therapies is crucial.1 Despite much headway, there is a mounting and continually evolving body of knowledge about this virus and its sequelae. While most symptomatic patients have a mild clinical course, approximately 20% require hospitalization, with upwards of 20% requiring an intensive care unit (ICU) transfer.2,3 Severe COVID-19 is characterized by clinical criteria and lung damage often seen concomitantly with high concentrations of circulating cytokines, including interleukin-6 (IL-6). This overproduction of cytokines and unregulated host response promote inflammation leading to cell damage otherwise known as cytokine storm. For patients with COVID-19, the number of immune cells and other inflammatory indices, particularly IL-6, are significantly higher among severely and critically ill patients. A high level of cytokines may also be associated with a worse prognosis.4
Baricitinib, a Janus kinase (JAK) inhibitor which modulates the production of cytokines to reduce inflammation, is gaining immense interest as a potential treatment option for hospitalized patients diagnosed with severe COVID-19. Historically this agent has been used for the treatment of rheumatoid arthritis (RA), with a U.S. Food and Drug Administration (FDA)-approved dose of 2 mg daily.5 Baricitinib inhibits JAK 1 and 2, which are involved in stimulating hematopoiesis and immune cell function through the signaling pathway.5 Inhibition of JAK prevents the activation of signal transducer and activator of transcription (STAT) proteins and reduces serum immunoglobulin (Ig) G, IgM, IgA, and C-reactive protein (CRP).6,7,8 Therefore, it prevents hyperinflammation (by reducing select inflammatory markers), improves lymphocyte counts, and improves oxygenation.
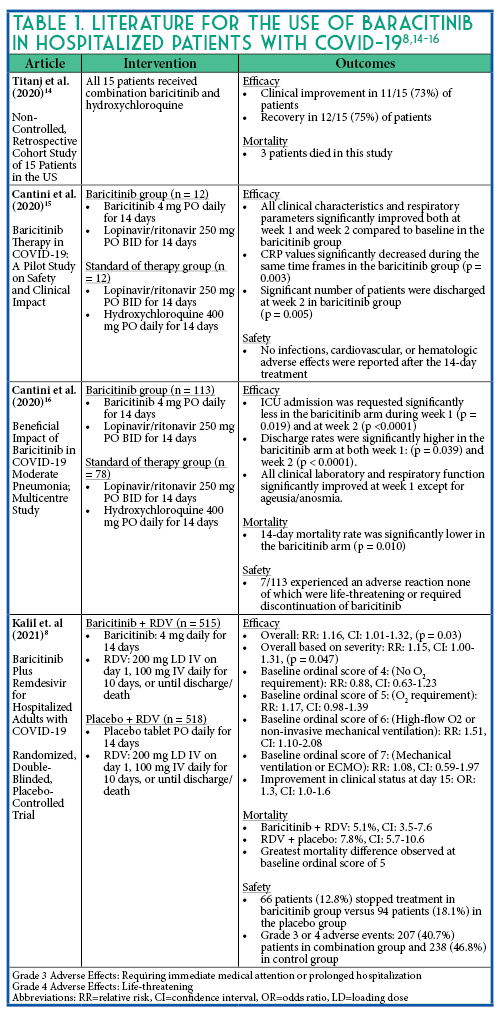
Additionally, JAK inhibitors prevent phosphorylation of key proteins involved in the signal transduction that leads to immune activation and inflammation (e.g., the cellular response to proinflammatory cytokines such as IL-6), as shown in Figure 1.9,10 With the ability to decrease inflammation by inducing immunosuppression, baricitinib possesses theoretical antiviral activity through interference with viral endocytosis, potentially preventing entry into and infection of susceptible cells.11 This mechanistic advantage led to clinical investigation of baricitinib as a potential therapy against SARS-CoV-2. Early evaluation was limited to retrospective cohort designs and non-controlled pilot studies as noted in Table 1. Initial interest prompted the inclusion of baricitinib as an investigational agent in the ACTT-2 trial. In this study, Kalil et al conducted a double-blind, randomized, placebo-controlled trial and demonstrated that baricitinib in combination with remdesivir (RDV) resulted in a reduced time to recovery (7 days vs. 8 days with placebo) and a 30% higher odds of clinical improvement by day 15 (OR 1.3, 95% CI 1.0-1.6). Those patients receiving supplemental high-flow oxygen or noninvasive mechanical ventilation demonstrated the greatest benefit with an even shorter time to clinical improvement (10 days vs. 18 days with placebo).8 In light of this evidence, the FDA issued an Emergency Use Authorization (EUA) in November 2020 for the use of baricitinib in combination with remdesivir in hospitalized patients with suspected or confirmed COVID-19 requiring supplemental oxygen. The role of baricitinib will be further investigated in combination with remdesivir compared to standard of care, dexamethasone plus remdesivir, in the currently enrolling ACTT-4 trial. One potential benefit of baricitinib is the reduction of profound immunosuppression that may be solicited compared to dexamethasone use.
.jpg)
Baricitinib EUA Information
Table 2 provides additional information regarding baricitinib therapy and a specific institution’s protocol for the treatment for COVID-19.
Safety Concerns for Baricitinib Use and COVID-19
Despite concerns about immunosuppression, secondary infections, and thrombosis with the use of JAK inhibitors, baricitinib was not associated with a significantly higher incidence of adverse events or thromboembolic events in the treatment of COVID-19.10 This may in part be due to its short half-life (~9-12 hours) and short duration of treatment, as more of the serious adverse effects have been reported after prolonged therapy. According to the ACTT-2 trial, the most common side effects seen with the acute use of combination baricitinib and RDV were hyperglycemia, anemia, decreased lymphocyte count, and acute kidney injury.8 Event rates were similar between baricitinib and placebo.
Conclusion
The combination of baricitinib, an anti-inflammatory medication, and RDV, an antiviral, reduced time to recovery of patients hospitalized with COVID-19, especially those requiring high-flow oxygen or non-invasive mechanical ventilation therapy. Future studies will evaluate the potential benefits of baricitinib compared to the current standard of care for the treatment of COVID-19. However, the combination of baricitinib plus RDV may benefit hospitalized patients requiring high-flow oxygen or non-invasive mechanical ventilation therapy who cannot otherwise tolerate corticosteroids.
References
- Centers for Disease Control and Prevention. CDC COVID Data Tracker. https://covid.cdc.gov/covid-data-tracker/ (accessed 2021 Feb 23).
- Docherty AB, Harrison EM, Green CA, et al. Features of 20 133 UK patients in hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: prospective observational cohort study. BMJ. 2020;369:m1985.
- Fu L, Wang B, Yuan T, et al. Clinical characteristics of coronavirus disease 2019 (COVID-19) in China: A systematic review and meta-analysis. J Infect. 2020;80:656-665.
- Tang Y, Liu J, Zhang D, Xu Z, Ji J, Wen C. Cytokine Storm in COVID-19: The Current Evidence and Treatment Strategies. Front Immunol. 2020.
- Baricitinib [monograph]. In: Lexicomp Online [online database]. Hudson, OH: Lexi-Comp (assessed 2020 Jan 6).
- Babon JJ, Lucet IS, Murphy JM, Nicola NA, Varghese LN. The molecular regulation of Janus kinase (JAK) activation. Biochem J. 2014;462:1-13.
- Bousoik E, Montazeri Aliabadi H. “Do We Know Jack” About JAK? A Closer Look at JAK/STAT Signaling Pathway. Front Oncol. 2018;8:287.
- Kalil AC, Patterson TF, Mehta AK et al., Baricitinib plus Remdesivir for Hospitalized Adults with Covid-19. Randomized, double-blind trial evaluating baricitinib plus remdesivir in hospitalized patients with Covid-19. New Engl J Med;2021.384(9):795-807.
- Zhang W, Zhao Y, Zhang F, et al. The use of anti-inflammatory drugs in the treatment of people with severe coronavirus disease 2019 (COVID-19): The perspectives of clinical immunologists from China. Clin Immunol. 2020;214:108393.
- Jorgensen S, Tse C, Burry L, Dresser L. Baricitinib: A Review of Pharmacology, Safety, and Emerging Clinical Experience in COVID-19. Pharmacotherapy. 2020;40:843-856.
- Stebbing J, Phelan A, Griffin I, et al. COVID-19: combining antiviral and anti-inflammatory treatments. Lancet Infect Dis. 2020;20:400-402.
- Food and Drug Administration. Commissioner of the U.S. Food and Drug Administration. http://www.fda.gov/ (accessed 2021 Feb 23).
- Remdesivir [monograph]. In: Lexicomp Online [online database]. Hudson, OH: Lexi-Comp (assessed 2020 Jan 6).
- Titanji BK, Farley MM, Mehta A, et al. Use of Baricitinib in Patients With Moderate to Severe Coronavirus Disease 2019. Clin Infect Dis. 2020:ciaa879.
- Cantini F, Niccoli L, Matarrese D, Nicastri E, Stobbione P, Goletti D. Baricitinib therapy in COVID-19: A pilot study on safety and clinical impact. J Infect. 2020;81:318-356.
- Cantini F, Niccoli L, Nannini C, et al. Beneficial impact of Baricitinib in COVID-19 moderate pneumonia; multicentre study. J Infect. 2020;81:647-679.
ICHP Best Practice Award
Applications must be received by July 1st. Visit our
website to apply online.
Program objectives and criteria
The objective of the program is to encourage the development of new, innovative pharmacy practice programs or innovative approaches to existing pharmacy practice challenges in health systems within the state of Illinois.
Applicants will be judged on their descriptions of programs and practices employed in their health system based on the following criteria:
- Innovativeness / originality
- Contribution to improving patient care
- Contribution to institution and pharmacy practice
- Scope of project
- Quality of submission
Eligibility
Applicants must be a member of ICHP for a minimum of 90 days prior to the submission deadline and practice in a health system setting. More than one program can be submitted by a health system for consideration.
Instructions for preparing manuscript
Each entry for the Best Practice Award must include a manuscript prepared as a Word document, double-spaced using Times New Roman 12-pitch type. A header with the paper title and page number should appear on each page.The manuscript should not exceed 2000 words in length (not counting references), plus no more than a total of 6 supplemental graphics (tables, graphs, pictures, etc.) that are relevant to the program. Each picture, graph, figure, and table should be mentioned in the text and prepared as a separate document clearly labeled.
The manuscript should be organized as a descriptive report using the following headings:
- Introduction, Purpose, and Goals of the program
- Description of the program
- Experience with and outcomes of the program
- Discussion of innovative aspects of programs and achievement of goals
- Conclusion
Format
Submissions will only be accepted via online submission form. The manuscript will be forwarded to a pre-defined set of reviewers. Please do not include the names of the authors or affiliations in the manuscript to preserve anonymity.
All applicants will be notified of their status within three weeks of the submission deadline. Should your program be chosen as the winner:
The program will be featured at the ICHP Annual Meeting. You will need to prepare a poster to present your program and/or give a verbal presentation. Guidelines will be sent to the winner.
You may be asked to electronically submit your manuscript to the ICHP KeePosted™ for publishing as a continuing pharmacy education home study program.
You will receive a complimentary registration to the ICHP Annual Meeting, recognition at the meeting and a monetary award distributed to your institution.
For more information
The 2021 Best Practice Award is sponsored by Krause Construction.
Features
PTCB Credentials & Certificates
Congratulations Techs!
The Pharmacy Technician Certification Board (PTCB) offers pharmacy technicians a wide range of certifications and certificates to help pharmacy technicians grow in their career.
Certifications:
- Certified Pharmacy Technician (CPhT)
- Certified Compounded Sterile Preparation Technician (CSPT)
- Advanced Certified Pharmacy Technician (CPhT-Adv)
Certificates:
- Medication History Certificate
- Technician Product Verification Certificate
- Hazardous Drug Management Certificate
- Billing and Reimbursement Certificate
- Controlled Substances Diversion Prevention Certificate
- Immunization Administration Certificate
ICHP would like to take a moment to recognize our Pharmacy Technician members who have worked hard to complete these programs and earn certifications and certificates, since their CPhT.
In order to earn a CPhT-Adv credential a technician must be active with PTCB, complete at least four certification programs (including Technician Product Verification and/or Medication History) – OR- three certificate programs AND PTCB’s CSPT Certification.
ICHP has four technician members who have earned this credential.
- Amanda Bentley
- Janice Nordmann
- Rebecca (Becky) Ohrmund
- Ellen Smith
We are so proud of the hard work and dedication that these technicians have shown in advancing excellence in pharmacy!
We would also like to recognize the technicians in our membership who have completed PTCB’s certification and certificate programs!
Certified Compounded Sterile Preparation Technician (CSPT)
Amanda Bentley
Emily Boyer
Temitope Fadonugbo
Peggy Janiszewski
Leslie Junkins
Sontha Lu
Joellyn Schefke
Ellen Smith
Medication History Certificate
Jessica Banks
Amanda Bentley
Johnathan Brooks
Aaron Macias
Kristine Mroz
Rebecca Ohrmund
Jennifer Santillan
Ellen Smith
Technician Product Verification Certificate
Aaron Macias
Kristine Mroz
Rebecca Ohrmund
Jennifer Santillan
Ellen Smith
Hazardous Drug Management Certificate
Ellen Smith
Billing and Reimbursement Certificate
Letrina Flowers
Aaron Macias
Kristine Mroz
Rebecca Ohrmund
Jennifer Santillan
______________________________________________________________________________________
Join the Pharmacy Technician Network!
Nominations Committee
On the Lookout for Leadership
Every year ICHP elects new members to its Board of Directors. As existing officers complete their terms, they often move into other leadership positions within ICHP. That means we’re always on the lookout for more pharmacy professionals to step into leadership roles within the organization.
This year is no exception. If you’ve been wanting to get more involved with ICHP, now’s your chance! With Carrie Vogler completing her term as Immediate Past President and several other offices up for election, there are several that will need candidates. Below is a list of the offices open for election in the Fall of 2021.
All the elected candidates will take office at the 2021 Annual Meeting with the exception of the President-elect, who assumes office immediately. So each new leader will have almost a year to train for their new job and be coached by our current Board Members. You don’t have to run that race unprepared! Job descriptions for each office may be found on the ICHP website at:
www.ichpnet.org/about_us/board_of_directors/job_descriptions/.
ICHP Board officers to be elected this fall:
- President-elect
- Secretary-elect
- Secretary (1 year term)
- Director-elect of the Division of Educational Affairs
- Director-elect of the Division of Marketing Affairs
- Technician Representative-elect
- Chair-elect of the New Practitioners Network
We also need to elect new officers for our affiliate chapters:
- NISHP – President-elect
- NISHP – Treasurer
- NISHP – Technician Representative
- Sangamiss – President-elect
- West Central – President-elect
- Sugar Creek - President
- Southern Illinois - President
- Metro East - President
- Rock Valley - President
If you are interested in running for an office or you would like to know more about an office before committing to run, you may contact the Committee on Nominations Chair, Carrie Vogler at
cvogler@siue.edu or Chris Crank at
chrisc@ichpnet.org. We hope you are ready to help lead the way for ICHP and Pharmacy!
Recognize The Best
ICHP Awards Process Opens
It's time to start thinking awards! ICHP is looking to honor the best and brightest in Illinois Pharmacy!
The award nominations process for the 2021 ICHP Pharmacist of the Year, New Practitioner Leadership Award, the Amy Lodolce Mentorship Award, the Industry Award and the Pharmacy Technician of the Year recipients are open, and it’s your chance to recommend someone you know and respect.
All five awards will be presented at the 2021 ICHP Annual Meeting on September 23-25, 2021 at the Drury Lane Theater in Oakbrook Terrace along with several other important awards. The criteria are different for each award, so take a look at the requirements! Deadline: July 1, 2021.
Pharmacist of the Year Award
A Pharmacist of the Year nominee should meet the following criteria:
- The nominee is a person of high moral character, good citizenship and high professional ideals;
- The nominee has made significant contributions affecting the practice of health-system pharmacy throughout the State; and
- These contributions should be in the form of sustained exemplary service in health-system pharmacy or a single outstanding achievement, or a combination of accomplishments benefiting health-system pharmacy, through it, humanity, and the public health. These accomplishments, achievements, or outstanding performances may be in the following areas:
- Health-system pharmacy practice
- Health-system pharmacy education
- Health-system pharmacy administration
- Pharmaceutical research or development related to health-system pharmacy
- Pharmacy organizational activity with a definite relationship to health-system pharmacy
- Scientific or professional pharmacy writing, (e.g., noteworthy articles on pharmaceutical subjects with applicability to health-
- system pharmacy)
- Pharmaceutical journalism related to health-system pharmacy
- Public and/or inter-professional relations activities benefiting health-system pharmacy
- Pharmacy law or legislation, professional regulations, standards of professional conduct or pharmacy law enforcement as related to health-system pharmacy.
Nominations may be received from Selection Committee members (past recipients of the award), past Presidents of the Council, affiliated chapters of the Council or any six pharmacist members of the Council submitting and signing a recommendation. Nominators should write a complete nomination letter and submit it along with the nominee’s CV by July 1st, to the ICHP office at
ChrisC@ichpnet.org.
Nominations should include the name of the nominee, name of the nominators, and details describing how the nominee meets the above criteria. This year’s Selection Committee Chair is last year’s recipient, Starlin Haydon-Greatting. All nominations will be forwarded to the ICHP office for distribution to the selection committee.
New Practitioner Leadership Award
The Illinois Council of Health-System Pharmacists establishes the New Practitioner Leadership Award to recognize an individual whose early accomplishments distinguish them as future leaders in the profession. The candidates should be individuals whose performance demonstrates a high degree of professionalism, leadership, and innovation. Nominations may be submitted to the ICHP Board of Directors sixty days prior to the Annual Meeting by an affiliate chapter or any two individual members of the ICHP. If a nominee is selected to receive the award, it will be presented at the Annual Meeting.
Nominees should meet the following criteria:
- Earned his/her first pharmacy degree within the last 10 years
- Encourage and support ICHP by membership, meeting attendance, and participation*
- Demonstrate a consistently high level of professional achievement
- Has developed, is working in or is working towards the development of an innovative practice in Health-System pharmacy practice
- Exhibit strong leadership qualities
- Possess a strong commitment to the advancement of the pharmacy profession
*Membership in ICHP and volunteer activity within ICHP’s divisions, committees or board of directors are absolute requirements to receive this award.
Selection of a recipient shall be by the ICHP Board of Directors in a secret ballot. The nominator may be requested to provide additional information to the ICHP Board of Directors to facilitate discussion and selection.
To apply or nominate, submit a detailed letter of recommendation identifying the specific accomplishments of the nominee with respect to each criteria above to
ChrisC@ichpnet.org.
Amy Lodolce Mentorship Award
Amy Lodolce was a University of Illinois at Chicago College of Pharmacy faculty member who touched the lives of pharmacy students, residents, and colleagues through her passion for teaching and the profession of pharmacy. Throughout her time at the college, Amy oversaw the training of four PGY2 drug information pharmacy residents, all of whom are currently drug information faculty at various institutions. She worked directly with numerous PGY1 residents and APPE students during their drug information rotations. She also served as a formal mentor to her student advisees and was the advisor of the Phi Delta Chi pharmacy fraternity for many years. As the Assistant Director of the Drug Information Group, Amy served as an informal mentor to other faculty and was quick to help new faculty become oriented and situated.
Amy approached being a leader and a mentor with an “open door” policy, and she would selflessly pause her work to address others’ needs. Students, residents, and faculty alike would ask her for guidance with career decisions and other professional concerns. Amy was respectful and nonjudgmental in her approach when assisting others whose goals and aspirations may have been different from her own. Her dedication was exemplary in that she worked tirelessly to provide residents and students with quality learning opportunities. She led and coached by example, consciously choosing behaviors that she hoped students and residents would emulate. An active pharmacist member of ICHP, Amy placed emphasis on professional organization involvement and giving back to the profession. Amy’s dedication and generosity to the profession of pharmacy have positively shaped many pharmacists’ careers, and the memory of her will continue to do so.
Award Criteria:
- The individual nominated to receive this award must be an ICHP pharmacist, associate or technician member in good standing;
- The individual should be an exemplary preceptor, professor and/or mentor of students, residents, pharmacy technicians and/or new practitioners;
- The individual should be a positive role model for pharmacists, pharmacy students and/or pharmacy technicians;
- In order to be considered for the award, individuals must have been nominated using the approved nomination form below;
- More than one person may complete a nomination form for an individual.
To nominate someone for the Amy Lodolce Mentorship Award:
Please provide your name(s), i.e., the name of the nominator(s). (More than one person can nominate a nominee).
Provide the name of the person you are nominating. In addition, the nominee’s curriculum vitae must be included in the nomination package.
Please answer the following questions about the nominee:
- Is the nominee a member of ICHP?
- In what capacity have you worked with the nominee?
- In what ways do you see the nominee working to advance the profession of pharmacy?
- Give some examples of ways in which this nominee is a model mentor/preceptor.
- Give some examples in which this nominee has demonstrated a service to community (outside of job responsibilities).
- How has this nominee impacted your career?
Industry award
The Illinois Council of Health-System Pharmacists establishes an Industry Award to recognize that individual from industry who over the years has made unique contributions to Health-System pharmacy in the state. Nominations may be submitted by an affiliate chapter or any two individual members of the ICHP. If a nominee is selected to receive the award, it will be presented at the Annual Meeting. Nominees should meet the following criteria:
The individual has made contributions to the practice of pharmacy in the state of Illinois beyond the scope of duty and responsibility.
The individual has been an effective liaison between Health-System pharmacy practitioners and the manufacturer enabling the manufacturer to respond to new developments in Health-System pharmacy practice.
The individual has encouraged and supported the ICHP over the years by membership, and meeting attendance and participation.
ICHP Technician of the Year Award
Award Purpose:
The ICHP Pharmacy Technician of the Year Award is established to identify and recognize exceptional performance by a certified pharmacy technician within the State of Illinois.
Award Criteria:
The candidate must:
- Be a current ICHP technician member,
- Be a PTCB certified pharmacy technician for at least two years,
- Demonstrate at least one of the following:
- exceptional contributions to his/her pharmacy worksite
- exceptional contributions to ICHP as a volunteer member
- exceptional contributions to the practice of pharmacy in Illinois
The nominator must:
- Be the technician’s supervisor, colleague, or co-worker. No self-nominations will be accepted.
- Provide the following information:
- Worksite name, address and telephone number.
- Technician name and year certified.
- Describe the technician’s contributions in detail.
- Provide the nomination to the ICHP office by no later than July 1st.
Selection Process:
- Deadline for nominations is July 1, 2021.
- All nominations are reviewed by the Division of Marketing Affairs at their July conference call.
- The Division will select two finalists for consideration and present them to the ICHP Board of Directors at the July Board Meeting.
- The ICHP Board of Directors will select the award winner from the two finalists presented by the Division of Marketing Affairs.
- The Division of Marketing Affairs may recommend one of the two finalists by providing detailed discussion points to the Board of Directors.
- The Board is not required to select a recipient if no candidate seems qualified.
- Award:
- The Award recipient and her/his nominator will be notified immediately following his/her selection by the Board of Directors.
- The award recipient will receive a complimentary full registration to the ICHP Annual Meeting.
- The award recipient will receive a plaque to be presented at an appropriately agreed upon time during the ICHP Annual Meeting.
Remember, the deadline for submissions of all award nominees is July 1, 2021.
Spring Meeting Recap
by Melissa Dyrdahl, BA; Communications Manager, ICHP
“Spring is the time of plans and projects.” – Leo Tolstoy1
What a joy it was to see the hours of planning and preparation blossom into the 2021 ICHP/MSHP Spring Meeting. Pharmacy professionals from across the Land of Lincoln and the Show Me State gathered together, virtually, on March 19 & 20, 2021 to “Build a Bridge – Create a Legacy”. This year’s meeting platform provided attendees with a fun, interactive lobby, complete with avatars bustling about – hopefully by our next meeting we’ll be able to mingle in person!
Speaking of mingling, we kicked off our meeting on Thursday with our Reverse Exhibit and Networking Mingle. The Reverse Exhibit featured 24 decision makers from Illinois and Missouri – 18 of those from Illinois alone, and 64 industry representatives. A reverse exhibit is when industry representatives have the opportunity to meet with the hospital/health-system directors whom they are interested in speaking with. This event brings in funds that help us keep meeting registration prices low – so THANK YOU to the directors who graciously gave of their time and to our industry partners who participated. We rounded off Thursday with the networking mingle. The relaxed forum allowed members from ICHP and MSHP to gather ‘face-to-face’ and catch up with one another – fun filters included.
Our continuing education started bright and early Friday morning with two opening sessions – one on managing burnout, another on advancing pharmacy technicians. This year’s keynote presentation was brought to us by ICHP members Abby Kahaleh and Rachael Prusi and focused on Public Health. During this time our exhibit hall was open – featuring nine digital booths for attendees to visit. The afternoon brought sessions on advocacy and law before breaking out into two more sessions – Best Practice presentations and a clinical session dealing with pediatric medication use. Poster presentations were available all meeting long though the ICHP website (see who won and read their abstracts in the KeePosted).
Saturday morning started with updates on Pharmacy Technician vaccine administration rules and our student session. Whether you’re a student or a well-seasoned pharmacy professional, Brooke Griffin’s presentation on cultivating your personal brand in pharmacy is definitely worth the watch. The morning also included presentations on ambulatory care and of course the COVID-19 pandemic. Past-president, Charlene Hope, presented an eye-opening talk on psychological safety, a topic that can be applied to every work setting. During the ICHP Town Hall Lunch, President Jen Arnoldi led a discussion on ASHP’s PAI 2030 Focused Initiatives, the pending requisite that pharmacy technicians be trained through a nationally accredited program, as well as ICHP’s COVID-19 resources.
The afternoon continued with presentations on COVID-19 vaccinations and treatment, antimicrobial stewardship, and our platform presentations (ICHP’s finalists were Caleb McLeod and Jaini Patel). In addition to all of our live and semi-live programs we were able to offer registrants six on-demand programs – plus all live programming was recorded for home study that attendees could watch at a later time.
“Legacy. What’s a legacy? It’s planting seeds in a garden you never get to see.” – Hamilton: An American Musical2
The theme of this meeting was “Build a Bridge – Create a Legacy”. One by one, credit by credit, pharmacy professionals spent the weekend learning and adding a few more beams to their bridge. We at ICHP feel honored to have been able to support you on this journey and look forward to seeing your legacies unfold!
Resources:
- https://www.goodreads.com/quotes/tag/spring
- https://www.theodysseyonline.com/top-20-favorite-quotes-hamilton-american-musical
Spring Meeting 2021: Poster & Platform Winners
You can view all of our poster presentations on the ICHP
website.
Other submissions include:
- Pharmacist Medication Review: An Integrated Team Approach to Service Home-Based Primary Care Patients
- Evaluation of Burnout Among Illinois Pharmacists
- Implementation of Virtual Rapid Sequence Intubation Kits to Reduce Potential Medication Exposure and Decontamination During the COVID-19 Pandemic
- A Statewide Professional Pharmacy Organization’s Approach to Raising Awareness of Diversity, Equity, and Inclusion in Pharmacy
- Incidence of Hypoglycemia Using 5 Units verus 10 Units of Regular Insulin in the Treatment of Hyperkalemia Patients in the Emergency Department
- Assessment of Medication History Accuracy and Completeness at Admission
- Comparison of a Centralized versus Decentralized Pharmacy Workflow in a COVID-19 Vaccination Clinic
- Assessment of Patient-Specific Risk Factors and Number of Medication Inconsistencies in a Primary Care Setting using Multidisciplinary Medication Reconciliation
- Illinois Drug Shortage Dashboard During the Coronavirus Disease 2019 (COVID-19) Pandemic
- Virtual Medication Tour with a Pharmacist as Part of a Cystic Fibrosis Telehealth Clinic
- Identification of Patient Factors Predictive of Naloxone Prescription: A Retrospective Cohort Study
- Synthesis of Truncated, Methanethiosulfonate-containing Analogues of ACHN-975
- Ketorolac Safety and Efficacy in Hospitalized Patients
Category: Original Research Poster Award Winner
Title: Clinical impact of rapid testing on gram negative bacteremia: A retrospective chart review
Abstract
Purpose:
Gram-negative bloodstream infections have been associated with poor patient outcomes including increased mortality. Rapid identification of microorganisms and resistance markers are valuable tools when it comes to targeting antimicrobial therapy. Molecular tests, used in conjunction with gram stain results, have the potential to reduce the time to organism identification and time to effective antibiotics. The objective of this study is to assess the impact of Verigene BC-GN on antimicrobial therapy-related outcomes. The primary outcome is time to first antibiotic intervention and time to most targeted therapy for gram-negative bloodstream infections pre- and post-implementation of rapid pathogen identification technology. Secondary outcomes include length of stay, use of antibiotics, 30-day readmission rate and mortality rate.
Methods:
This is a retrospective, single-center, cohort study assessing patients 18-89 years of age with gram-negative bacteremia from July 1st, 2018 to July 31st, 2020. The control group will consist of patients with a positive blood culture caused by a gram-negative pathogen from July 1st, 2018 to May 31st, 2019; prior to the implementation of Verigene assays. These patients will be compared to positive blood cultures from August 1st, 2019 to July 31st, 2020; post implementation of Verigene assays at Memorial Medical Center (MMC). Subjects will be excluded from review if they were transferred to MMC from outlying hospital due to need for higher level of care, deceased/hospice care at time of positive blood culture result, secondary infections with differing cultures/susceptibilities or on additional antimicrobial therapy for concurrent infection with no cultures/sensitivities available.
Results: Research in Progress
Conclusions: Research in Progress
Submitting Author: Shelby Lynn Dial, PharmD, PGY-1 Pharmacy Practice Resident
Organization: Memorial Medical Center
Co-authors: Julie Downen, Pharm.D., BCPS, BCIDP, CLSSBB, Memorial Medical Center; Maithili Deshpande, PhD, Southern Illinois University Edwardsville
_______________________________________________________________________________
Category: Encore Poster Award Winner
Title: Impact of an Embedded Pharmacist on Diabetes Control in a Primary Care Practice
Abstract
Purpose/background:
In June 2019, 42% of patients with diabetes in Northwestern Medicine Regional Medical Group Wheaton Internal Medicine (IM) practice had a baseline glycated hemoglobin (HgbA1c) of >7.0%. The American Diabetes Association (ADA) goal for most adults with diabetes is an HgbA1c of < 7.0%. Diabetes is the 7th leading cause of death in the United States and uncontrolled diabetes can lead to major health complications. The UK Prospective Diabetes Study (UKPDS) found that every 1% reduction in HgbA1c was associated with a 37% decrease in microvascular disease and a 14% reduction in myocardial infarction (MI). Management of diabetes in primary care is complex and requires a multidisciplinary care team approach. For our project, we wanted to see if an embedded pharmacist in the Wheaton Internal primary care practice could reduce HgbA1c values by at least 0.5% in 30% of patients with diabetes with HgbA1c >7% by the end of fiscal year 2020. As a secondary outcome, we evaluated the impact of pharmacist services on provider burnout and patient satisfaction.
Methods:
We introduced a full-time embedded pharmacist to the care team at Wheaton IM to provide services to all patients with diabetes with an HgbA1c >7% via a signed collaborative practice agreement with all six providers in the practice. The clinical pharmacist recorded all medication interventions per patient. The project team used this intervention log as a basis to create automated reports on HgbA1c reduction and emergency department/hospitalization avoidance. In addition, we established pharmacist follow up criteria, identifying frequency of follow up for medication titration and various education needs
Results: 80.5% of patients with diabetes at the Wheaton IM practice decreased their HgbA1c by ≥0.5% after a clinical pharmacist was added to the patient care team. The most common pharmacist interventions included ensuring that the patient was on appropriate drug therapy, able to obtain their medications, and had access to proper disease state education. Additionally, this project led to a 38.6% decrease in provider burnout score, while achieving a 96.4% average patient satisfaction score. Lastly, a reduction in preventable diabetes-related emergency department visits of 95.1% and hospitalizations of 97.3% resulted in $85,965 in cost avoidance to Northwestern Medicine.
Conclusions: Adding a clinical pharmacist to the patient care team improved clinical outcomes, reduced health care spending, increased patient access to care, and reduced provider burnout. The keys to success were clearly defined pharmacist services, management of patient drug therapy, essential disease state education, establishment of patient follow-up criteria, and reduced demands on physician time. Next steps include implementing billing for pharmacist services and growing the program to include pharmacist presence in additional primary care practices.
Submitting Author: Imran Khan, PharmD, Clinical Pharmacist, Ambulatory Care Management
Organization: Northwestern Medicine Physician Network
Co-author: Therese Castrogiovanni, Pharm.D, CDCES, RMG Wheaton Internal Medicine.
_______________________________________________________________________________
Category: Student Poster Award Winner
Title: Rocuronium vs succinylcholine in the traumatically injured brain: a prospective, pilot study
Abstract
Purpose:
The purpose of this study was to assess the safety between two common paralytics, administered during rapid sequence intubation (RSI), in patients presenting with an acute traumatic brain injury (TBI) in the emergency department (ED). In these patients, RSI is implemented to protect a patient’s compromised airway. Following pharmacologic induction of a RSI, patients’ muscle tone is inhibited with rapid-onset, relatively short-acting paralytics such as rocuronium or succinylcholine. A retrospective study using rocuronium for RSI demonstrated mortality benefit in these patients. This prospective study compared the safety outcomes in similar patients who underwent RSI with either rocuronium or succinylcholine.
Methods:
Patients were identified for study inclusion between September 1, 2018 and June 30, 2020. The study population consisted of acute TBI patients who presented to the ED and required RSI using the paralytics succinylcholine or rocuronium. Demographics recorded include age, sex, race, severity of the TBI, and presenting Glasgow Coma Scale (GCS). Patients were excluded from the study if they were under the age of 18, a surgical airway was placed, patient was pregnant at time of study, cardiac arrest occurred prior to intubation, or intubation was attempted prior to arrival. The primary clinical outcome evaluated was the incidence of in-hospital mortality. The secondary outcomes measured both hospital and intensive care unit (ICU) length of stay (LOS), respectively. A sample size of 200 was calculated to detect a 20% difference in mortality.
Results: Presented at the Spring Meeting
Submitting Author: Nadine Alwawi, PharmD Candidate
Organization: Rosalind Franklin University of Medicine and Science
Co-authors: Lauren Stambolic, PharmD, Advocate Christ Medical Center; Marc McDowell, PharmD, BCPS, Advocate Christ Medical Center; Sabrin Jaber, PharmD, Stanford University Medical Center; Brook Walsh, PharmD, Little Company of Mary Hospital; Ellen Omi, MD, Advocate Christ Medical Center; Robert Mokszycki, PharmD, BCPS, University of Massachusetts.
_______________________________________________________________________________
Category: Original Research
Title: Evaluation of Bolus vs. Continuous Infusion Neuromuscular Blocking Agents in the Management of Severe Acute Respiratory Distress Syndrome
Abstract
Purpose:
Acute respiratory distress syndrome (ARDS) is characterized by pulmonary edema, reduced lung compliance, and acute hypoxemia following lung insult. The primary management of ARDS is lung protective ventilation to reduce the risk of barotrauma and volutrauma and exacerbation of lung injury. Neuromuscular blocking agents (NMBA) are often considered in patients with ARDS to manage ventilator dyssynchrony. Prior to March 2020 at Rush University Medical Center, continuous NMBA infusions were administered at a flat infusion rate according to the ACURASYS trial. Due to the large number of patients with COVID-19 infection who progressed to severe ARDS, NMBA dosing was re-evaluated to manage drug supply and prevent prolonged paralysis. NMBA order sets were updated to encourage initial intermittent bolus NMBA administration for ventilator dyssynchrony followed by a weight-based infusion for persistent or recurrent dyssynchrony. This MUE was designed to evaluate the use of bolus and weight-based continuous infusion NMBAs used in the management of ARDS associated ventilator dyssynchrony in COVID-19 positive patients.
Methods:
COVID-19 positive patients with orders for cisatracurium or rocuronium and a diagnosis of ARDS from March 1, 2020 through May 1, 2020 were identified for inclusion. Patients were included if they received at least one dose of either cisatracurium or rocuronium for ventilator dyssynchrony, define as a respiratory rate of at least 5 breaths per minute above the desired ventilator rate. Patients were evaluated for improvement in ventilator dyssynchrony by an improvement in respiratory rate, defined as a reduction of at least five breaths per minute; decreased peak inspiratory pressure, defined as a decrease in the peak inspiratory pressure of at least 5 cm H2O; or an improvement in the PaO2:FiO2 of at least 20 mmHg. Respiratory rate, ventilator rate, and peak inspiratory pressure were assessed by the most recent values available prior to NMBA administration and by the first result available at least 1 hour after administration. PaO2:FiO2 was assessed by arterial blood gas within 4 hours before and after NMBA administration. Duration and average rate of infusions were utilized to determine overall exposure in patients who received infusions.
Results:
Fifty-five patients had orders placed for either cisatracurium or rocuronium during the evaluation period. Three patients were excluded because they did not receive a dose of either cisatracurium or rocuronium and one patient was excluded because their encounter occurred at an outside facility. Patients were separated into the initial bolus group, those who received a bolus with at least one-hour separation from any subsequent infusion, and initial infusion group, those who received either no bolus or had les than one-hour separation between initial bolus and initiation of infusion. The overall response rate was 74.3% and 56.3% in the initial bolus and initial infusion groups respectively. In the initial bolus group, 57.1% of patients required a continuous NMBA infusion, and in the initial infusion group 68.8% of patients received at least one bolus. The median and mean overall cisatracurium exposure was 145 mg and 594 mg in the initial bolus group and 704 mg and 750 mg in the initial infusion group. Both strategies resulted in lower cumulative exposure of 1800 mg for the historic flat infusion rate. 4.
Conclusions:
Patients who received an initial bolus NMBA did not have less improvement in ventilator dyssynchrony compared to patients who received an initial infusion. Cumulative exposure associated with an initial bolus regimen was lower when compared to an initial infusion regimen. An initial bolus NMBA strategy may prove beneficial in reducing overall NMBA use in the management of ARDS, especially in the event of future drug shortages.
Submitting Author: Caleb McLeod, PharmD, PGY-1 Pharmacy Practice Resident
Organization: Rush University Medical Center
Co-author: Georgeanna Rechner-Neven, PharmD, BCPS, BCCCP, Rush University Medical Center.
College Connection
Midwestern University College of Pharmacy, Downers Grove
Independent Pharmacies: The Overlooked Health Source
by Ruba Samara, PharmD Candidate, Midwestern University College of Pharmacy, Student Chapter President
When I was 5 years-old, I would hear stories from my mother of her days working as a pharmacy technician at an independent pharmacy in Kuwait. She would boast about her workdays in the pharmacy and her love for her white coat. My passion for pharmacy began as a child, and it grew through my mother. My mother had a dream of helping others, and I soon realized that I shared that dream. As an undergraduate student, I studied biology, which helped me grow fonder of the human body. Learning new processes of the human body at the cellular level helped push me towards a career in the medical field, and it helped prepare me to become a student pharmacist.
While studying as an undergraduate student, I chose to work in a pharmacy setting that allowed me to develop a relationship with my patients to deliver the best patient care possible and the best health outcomes. I accepted a position at an independent pharmacy located at the Little Company of Mary Outpatient Center in Evergreen Park. Through working at an independent pharmacy in an urban community, I recognized the weak and unestablished health education infrastructure. I realized that our pharmacy's patient population had a profound health literacy issue, and I also realized that the many medical compliance problems stemmed from a lack of knowledge. This motivated me to team up with pharmacists and physicians to provide education sessions to lead our patients toward healthy lifestyles through proper understanding. Although our pharmacy team was small, we had astonishing results and noticeable improvements in our patient population.
Along with having a positive impact within the local community, working at an independent pharmacy improved my interprofessional skills through the idea of integrated health. Although we are an outpatient pharmacy, we work directly with the inpatient staff to deliver medications to patients discharged from the hospital. I work with social workers to check patient coverage on medications such as DOACs, and I can work with doctors to find better alternatives that are less costly for the patient. I also provide counseling to the patients regarding their new medications and help them better understand their disease states. After all, pharmacists are the most accessible health care professionals, and we follow through with the patient until the end.
While enjoying my work experiences at the Evergreen Park independent pharmacy, I also began working at two other locations. The pharmacies were located inside health clinics, which helped strengthen my ability to interact with healthcare providers of various backgrounds. I enjoyed working at each of these sites because of the clinical setting, which allowed for a more interdisciplinary network. This allowed me to pursue my goal of optimizing patient care. While working, I can ask questions regarding medications while learning the indication and pharmacology of each drug. I can share my knowledge during each patient interaction as I improve my patient communication skills.
The COVID-19 pandemic has posed a new threat to independent pharmacies as well as vulnerable communities. Many retail chains have become vaccination sites and have been given access to the vaccines. Meanwhile, independent pharmacies are still waiting to be added as vaccination sites. The pandemic has hit many urban communities the hardest, and their best healthcare access is independent pharmacies. We are part of the community, and many patients trust us to ensure patient care delivery whenever they need it. We hope to continue to impact the community and our patients positively; however, we are currently overlooked by the state. As a pharmacy student, I took an oath to protect my patients and care for them. I hope that sometime soon, I can provide my patients with the COVID-19 vaccine they need to walk around safely in the neighborhood. I will continue to bring awareness to independent pharmacies to optimize patient care for our communities.
Southern Illinois University Edwardsville School of Pharmacy
The 2021 Faculty Auction
by Sara Gardner, P2, Student Chapter President-Elect, SIUE School of Pharmacy
The annual “faculty auction” is an exciting event that the SIUE SSHP chapter hosts each spring. It is both a fundraiser for our organization and an excellent way for students and faculty to get to know one another on a more personal level. During this event, students are invited to bid on activities or prizes that faculty members offer. Our chapter donates a portion of the profits from this event to charity, which has included the Ronald McDonald House Charities of Metro St. Louis for several years. Like many past events, our auction has traditionally taken place in person, but the COVID-19 pandemic has caused the need for it to be transitioned to an online format. Thanks to our executive board members' hard work, this transition occurred seamlessly last year, and we’re looking forward to holding this event via Zoom again this spring!
To plan the faculty auction effectively, our executive board members are each assigned several professors to contact about the auction. If a professor is interested in participating, they provide details about the prize they will offer up for bidding. Faculty members create prizes that may include a personal interest of theirs - which is part of what makes this event so much fun! Prizes can be proposed individually or by groups of faculty members. They may also allow for more than one student to participate, therefore students often plan to bid on an event that they would like to do as a group. A student volunteer or member of our executive board acts as the Master of Ceremonies for the auction and starts the bidding for each prize at a particular amount. Each item increases in price until only one student or group remains with the amount they wish to bid. Past prizes have included donations from many faculty members, including our chapter’s faculty advisors, Dr. Jingyang Fan and Dr. Keith Hecht, who have donated a “foodie tour” for years, including a sampling of St. Louis cuisine and a BBQ tour. Dr. Fan says, “It is a great way to get to know students on a personal level, discuss likes and dislikes of food, share BBQ techniques, all while filling our stomachs with amazing food! We look forward to doing the BBQ tour again this year.” Dr. Lisa Lubsch has also donated many prizes to the auction. She says, “I miss concerts, but I enjoy reflecting on previous St. Louis events students have attended with me, including a St. Louis Cardinals game and a Red Hot Chili Peppers concert!” Prizes from other faculty have included an escape room experience, a day of boating, faculty hangouts, a virtual pizza and game night, gift baskets, and even a spring cleaning!
The faculty auction is an “outside of the box” way for our organization to fundraise and a way for teachers and students to have fun experiences together outside of class. The offered activities have helped create positive relationships between the SIUE School of Pharmacy faculty and students, and the auction is highly anticipated each year. We hope this tradition continues for years to come!
University of Illinois Chicago College of Pharmacy
Continuing Innovation Through The Pandemic
by Maxwell Stone, P3, Student Chapter Co-President Rockford Campus, University of Illinois Chicago College of Pharmacy
During the past year, we have all seen significant changes to the way we practice pharmacy. The COVID-19 pandemic has caused changes to our protocols, relocations to remote and online environments, new medication utilization, new drug shortages, and increased demand for PPE. Pharmacy practice was rapidly evolving before the virus became omnipresent. The 2020 ASHP Pharmacy Forecast had a lot to say about how hospital and health system pharmacy may change.1
Innovation is often synonymous with new technology. This year’s Pharmacy Forecast discussed advanced computing technologies and the application of genomics. Artificial intelligence and advanced computing technologies have the potential to aid or even replace pharmacists in some patient-care-related tasks as they progress. There are still many barriers to implementing Artificial Intelligence, such as standardizations in data collection or data sources within EHRs. Genomics has been a hot topic in pharmacy for some time now. This year's edition of the Pharmacy Forecast discussed the ethical use of genomic testing, strategic recommendations for practice leaders, and genetic modification therapies. Gene therapy is quickly growing and covers many different clinical applications.
I had the opportunity to talk with the pharmacy team at SwedishAmerican Hospital, a UW Health division, about how their hospital is taking innovations one step further. The pharmacy has implemented BoxPicker® (an automated pharmacy storage and retrieval system) and Kit Check® (an automated medication tray and cart management system). I spoke with Pharmacy Director, Tom Carey and PGY1 Pharmacy Resident, Dayna Redini, UIC COP Class of 2020, about pharmacy innovations with Kit Check®.
Kit Check® is a tool designed to improve efficiency, patient safety, and medication visibility for medication trays and carts. Kit Check® uses RFID tags to scan and track medications quickly. Once medications are appropriately tagged, the Kit Check® scanning station can scan a tray to quickly create an inventory report indicating which medications are missing, expiring, or placed incorrectly. Kit Check® is designed to make the entire scanning, re-stocking, and verification process faster and more streamlined.
SwedishAmerican is utilizing Kit Check® as an inventory monitoring system and reducing workload in re-stocking trays. The management system has been incorporated in the re-stocking of anesthesia trays, GI trays, L&D trays, and crash carts. Dayna tells me, “The goal is to modernize our inventory tracking, decrease the workload of technicians and pharmacists, and reduce medication errors.” It is too early to see any data in cost-saving, but the pharmacy is already using utilization data to reduce the par of medications that are not routinely used. This helps save re-stocking time and reduces inventory.
The technology takes some time to install and set up with the pharmacy director, inpatient manager, and IT manager's cooperation. There is also the substantial groundwork involved in preparing all the medications, labeling thousands of medications, and entering them into the system. Complete implementation of the system, including training and adjustments to procedures, took a few months.
Training is an essential component of any new process. SwedishAmerican ensured that each employee had personal, hands-on training to understand the new processes better. The pharmacy team is trained so that the new system can be utilized appropriately and keep the patients safe. Throughout the training, some complications were identified, and adjustments were made to procedures. The most considerable complications were phasing out the old system and clearing up the confusion.
Several UIC students had the opportunity to work hands-on with Kit Check®. The training is fast and efficient, taking only about 15 minutes. Checking a tray for a crash cart takes only about 2 minutes. SwedishAmerican is always looking to innovate by incorporating technology to help serve our patients. We are all excited to see what innovations in healthcare are coming next.
References
- Vermeulen LC, Swarthout MD, Alexander GC, et al. ASHP Foundation Pharmacy Forecast 2020: Strategic Planning Advice for Pharmacy Departments in Hospitals and Health Systems. Am J Health-System Pharm. 2020:77(2);84–112. https://doi.org/10.1093/ajhp/zxz283
More
Upcoming Events
Sangamiss Live Webinar & Meeting (Virtual)
May 11, 2021
Topic: Oncologic Emergencies: Staying Calm with Clinical Updates
Speaker: Lucas Beckman, PharmD
Accredited for health-system pharmacists
CE Appetizer Live Webinar & Meeting (Virtual)
May 13, 2021
Topic: Is PO a Go? Oral Step-Down Therapy in Enterobacterales Bacteremia
Speaker: Claire C. Schumann, PharmD
Accredited for health-system pharmacists
NISHP Live Webinar & Meeting (Virtual)
May 20, 2021
Topic: 340B Explained for Pharmacists and Pharmacy Technicians
Speakers: Thomas Yu, PharmD; Amita B. Patel, CPhT
Accredited for health-system pharmacists and pharmacy technicians
CE Appetizer Live Webinar & Meeting (Virtual)
June 9, 2021
Topic: Masking: Protecting Me and/or You?
Speaker: Mary Ann Kliethermes, BS, PharmD
Accredited for pharmacy technicians
PAC Trivia Night (Virtual)
June 3, 2021
Save the date - more details to follow
CE Appetizer Live Webinar & Meeting (Virtual)
July 14, 2021
Topic: Social Determinants of Health (SDOH) Factors on Medical Use and Health Outcomes
Speaker: Klodiana Myftari, PharmD, BCACP
ICHP Annual Meeting
September 23-25, 2021
Drury Lane Theatre & Events
Oakbrook Terrace, IL
Regularly Scheduled Conference Calls
- Educational Affairs
3rd Tuesday of each month - 11:00 am
- Executive Committee
1st Tuesday of each month - 8:00 am
- Government Affairs
3rd Monday of each month - 4:00 pm
- Marketing Affairs
3rd Tuesday of each month - 8:00 am
- Organizational Affairs
4th Monday of each month - 1:00 pm
- Professional Affairs
4th Tuesday of each month - 3:00 pm
Regularly Scheduled Network Meetings
- Ambulatory Care Network
1st Thursday of each month - 12:00 pm
- Chicago area pharmacy directors network dinner meeting
See ICHP calendar for details
www.ichpnet.org/events/calendar/
- New Practitioners Network
3rd Wednesday of each month - 4:00 pm
- Pharmacy Informatics and technology network
2nd Friday of every other month - 8:00 am
- Pharmacy Technician Network
2nd Tuesday of every other month - 5:00 pm
- Residency Leaders Network
3rd Friday of every other month - 2:00 pm
- Small and Rural Hospitals Network
See ICHP calendar for details
www.ichpnet.org/events/calendar/
Welcome New Members!
Welcome new members!
ICHP Pharmacy Action Fund Contributors
Thank you to everyone who has donated to the PAC!
ICHP Board of Directors 2021-2022
If you would like to contact a board member, please visit our
website.
Print Entire Issue




.jpg)



 resized.jpg)