Official Newsjournal of the Illinois Council of Health-System Pharmacists

November 2021
Volume 47 Issue 4
Columns
ICHP Leadership Spotlight Interview - Meet Brian!
ICHP Leadership Spotlight Interview - Meet Andrew!
Features
Collaborative Pharmaceutical Task Force Report - June
Collaborative Pharmaceutical Task Force Report - July
PTCB'S Recertification Process is Now Easier and Faster
Join us for the 2019 ICHP Annual Meeting
College Connection
Midwestern University Chicago College of Pharmacy
Roosevelt University College of Pharmacy
Rosalind Franklin University College of Pharmacy
Southern Illinois University Edwardsville School of Pharmacy
University of Illinois at Chicago College of Pharmacy
More
KeePosted Info
Illinois Council of Health-System Pharmacists
4055 North Perryville Road
Loves Park, IL 61111-8653
Phone: (815) 227-9292
Fax: (815) 227-9294
ichpnet.org
KeePosted
Official News journal of the Illinois Council of Health-System Pharmacists
EDITOR
Jennifer Phillips
ASSISTANT EDITOR
Milena McLaughlin
MANAGING EDITOR
Scott Meyers
ASSISTANT MANAGING EDITOR
Trish Wegner
DESIGN EDITOR
Melissa Dyrdahl
ICHP Staff
EXECUTIVE VICE PRESIDENT
Scott Meyers
VICE PRESIDENT - PROFESSIONAL SERVICES
Trish Wegner
DIRECTOR OF OPERATIONS
Maggie Allen
INFORMATION SPECIALIST
Heidi Sunday
CUSTOMER SERVICE AND
PHARMACY TECH TOPICS™ SPECIALIST
Jo Ann Haley
ACCOUNTANT
Jan Mark
COMMUNICATIONS MANAGER
Melissa Dyrdahl
LEGISLATIVE CONSULTANTS
Liz Brown Reeves
Mitch Schaben
ICHP's Mission Statement
Advancing Excellence in Pharmacy
ICHP's Vision Statement
ICHP dedicates itself to achieving a vision of pharmacy practice where:
· Pharmacists are universally recognized as health care professionals and essential providers of health care services.
· Pharmacists use their medication expertise and leadership skills to optimize the medication use process and patient outcomes.
· Pharmacy technicians are trained and PTCB certified to manage the medication distribution process.
ICHP's Goal Statements
· Raising awareness of the critical role pharmacists fulfill in optimizing medication therapy and ensuring medication safety in team-based, patient-centered care.
· Providing high quality educational services through innovative continuing pharmacy education and training programs, and sharing evidence-based best practices.
· Developing and nurturing leaders through mentorship, skill development programs, and leadership opportunities.
· Working with national and state legislators and policymakers to create or revise legislation and regulation critical to pharmacy practice and quality patient care.
· Urging pharmacy technician employers to require successful completion of an accredited pharmacy technician training program and PTCB certification of all pharmacy technicians.
Approved by the ICHP Board of Directors May 30, 2018.
KeePosted Vision
As an integral publication of the Illinois Council of Health-System
Pharmacists, the KeePosted newsjournal will reflect its
mission and goals. In conjunction with those goals, KeePosted will
provide timely information that meets the changing professional and personal
needs of Illinois pharmacists and technicians, and maintain high publication
standards.
KeePosted is an official publication of, and is copyrighted by, the
Illinois Council of Health-System Pharmacists (ICHP). KeePosted is
published 10 times a year. ICHP members received KeePosted as
a member benefit. All articles published herein represent the opinions of the
authors and do not reflect the policy of the ICHP or the authors’ institutions
unless specified. Advertising inquiries can be directed to ICHP office at the
address listed above. Image disclaimer: The image used in the Pharmacy Tech
Topics™ advertisement is the property of © 2017 Thinkstock, a division of Getty
Images. Some images are property of © 2019 Adobe Stock.
Copyright © 2019, Illinois Council of Health-System Pharmacists. All rights
reserved.
Columns
 Directly Speaking
Directly Speaking
The Measles: I've Had Them, You and Your Kids Don't Want Them!
by Scott A. Meyers, Executive Vice President
120x120.jpg) President's Message
President's Message
Making Your Impact Last
by Noelle Chapman, PharmD, BCPS, FASHP - ICHP President - Vice President, Pharmacy Operations - Advocate Aurora Health
- The Educational Affairs and Marketing Affairs Divisions have been encompassing technician and New Practitioner needs to address member engagement (ICHP currently has the highest technician membership of all time!)
- There has been consistent participation in the Collaborative Pharmaceutical Task Force meetings (a committee whose aim is to provide recommendations regarding the rewriting of the Pharmacy Practice Act due by the end of this year) and the Government Affairs Division has been diligently tackling legislative issues through our new lobbyists to ensure we are addressing the advocacy needs and concerns of our membership.
- An Executive Vice President Search Committee is currently working to make sure we have a sustainable plan for the leadership of our organization.
Given this direction, we have also been able to contemplate how we can do a little spring cleaning to provide space for us to continue to grow and develop as an organization and a profession. An IMPACT is essential to start the process, but it is just as important to take the direction provided by the IMPACT and ensure it is sustainable. I have been thinking a lot lately about viability. Viability is the ability to survive or live successfully. This is important when you want your IMPACT to live on, knowing it needs to be nimble and adjust to whatever is coming your way.
Board of Pharmacy Update
Highlights of the July 2019 Meeting
by Scott A. Meyers, Executive Vice President
Government Affairs Report
Fourteen Pharmacy Bills Make It Through!
by Scott A. Meyers, Executive Vice President
|
Bill Number |
Sponsor |
Summary |
Location |
|
SJRCA0001 |
Harmon – Oak Park, D |
Proposes to amend the Revenue Article of the Illinois Constitution. Removes a provision that provides that a tax on income shall be measured at a non-graduated rate. Provides that there may be one tax on the income of individuals and corporations (currently, there may be no more than one income tax imposed on individuals and one income tax imposed on corporations, and the rate of tax imposed upon corporations shall not exceed the rate imposed on individuals by more than a ratio of 8 to 5). Provides that the income tax may be a fair tax where lower rates apply to lower income levels and higher rates apply to higher income levels. Provides that no government other than the State may impose a tax on or measured by income. Effective upon being declared adopted. |
Adopted by both chambers
|
|
SB1135 |
Harmon – Oak Park, D |
Amends the Hospital Licensing Act. Permits hospitals that admit patients for treatment of mental illness to grant medical staff privileges to licensed prescribing psychologists. Amends the Clinical Psychologist Licensing Act. Requires a psychologist applying for a prescribing psychologist license to have completed 30 psychology doctoral graduate credit hours and 31 credit hours in a Master of Science degree program. Provides that clinical rotation training requirements for prescribing psychologists shall be completed under the administrative supervision of a Director or other faculty member of a regionally approved University that provides training for the master's degree in clinical psychopharmacology. Requires the clinical rotation training to be housed in a healthcare setting and to meet certain academic standards. Provides that all prescriptions written by a prescribing psychologist must contain the prescribing psychologist's name and signature. Provides that physicians may provide collaboration and consultation with prescribing psychologists via telehealth. Permits persons who have 5 years of experience as a prescribing psychologist in another state or at a federal medical facility to apply for an Illinois prescribing psychologist license by endorsement. Makes changes to the Clinical Psychologists Licensing and Disciplinary Board. Amends the Telehealth Act. Expands the definition of "health care professional" to include prescribing psychologists. Amends the Illinois Public Aid Code. Requires the Department of Healthcare and Family Services to reimburse prescribing psychologists for behavioral health services provided via telehealth. Requires the Department to, by rule, establish rates to be paid for specified services provided by clinical psychologists and prescribing psychologists. Effective immediately. |
Passed both Houses |
|
SB1250 |
Murphy – Des Plaines, D |
Amends the School Code. Requires a school district, public school, or nonpublic school to permit a student diagnosed with a pancreatic insufficiency to self-administer and self-manage his or her pancreatic enzyme replacement therapy if the parent or guardian of the student provides the school with written authorization for the self-administration or self-management and written authorization for the therapy from the student's physician, physician assistant, or advanced practice registered nurse; defines terms. Requires each school district or school to adopt an emergency care plan and develop an individualized health care plan for a student subject to the provision; specifies plan requirements. Provides that any disclosure of information under the provision shall not constitute a violation of the federal Health Insurance Portability and Accountability Act of 1996 or any regulations promulgated under that Act. Provides that any records created under the provision must be maintained in a confidential manner consistent with the federal Health Insurance Portability and Accountability Act of 1996. |
Passed both chambers |
|
SB1665
Same as HB2439 |
Hastings – Frankfort, D |
Amends the Illinois Controlled Substances Act concerning the Prescription Monitoring Program. Excludes licensed veterinarians from the reporting requirements under the Program. Provides that a licensed veterinarian shall report information required under the Prescription Monitoring Program if the person who is presenting an animal for treatment is suspected of fraudulently obtaining any controlled substance or prescription for a controlled substance to the Department of Human Services. Provides that a licensed veterinarian may not be subject to any licensure or disciplinary action by the Department of Financial and Professional Regulation for the failure to report such a person. Effective immediately. |
Passed both chambers |
|
SB1696 |
Steans – Chicago, D |
Amends the Medical Assistance Article of the Illinois Public Aid Code. Provides that during the first quarter of State Fiscal Year 2020, the Department of Healthcare of Family Services must convene a technical advisory group consisting of members of all trade associations representing Illinois skilled nursing providers to discuss changes necessary with the federal implementation of Medicare's Patient-Driven Payment Model. Provides that implementation of Medicare's Patient-Driven Payment Model shall, by September 1, 2020, end the collection of the MDS data that is necessary to maintain the current RUG-IV Medicaid payment methodology. Requires the technical advisory group to consider a revised reimbursement methodology that takes into account transparency, accountability, actual staffing as reported under the federally required Payroll Based Journal system, changes to the minimum wage, adequacy in coverage of the cost of care, and a quality component that rewards quality improvements. Effective immediately. |
Passed both chambers |
|
SB1715 |
Hastings – Frankfort, D |
Amends the Pharmacy Practice Act. Provides that the "practice of pharmacy" includes the administration of injections of long-term antipsychotic medications pursuant to a valid prescription by a physician licensed to practice medicine in all its branches, upon completion of appropriate training, including how to address contraindications and adverse reactions set forth by rule, with notification to the patient's physician and appropriate record retention, or pursuant to hospital pharmacy and therapeutics committee policies and procedures. |
Passed both chambers |
|
SB1828 |
Bush – Grayslake, D |
Creates the Needle and Hypodermic Syringe Access Program Act. Provides that persons or entities that promote scientifically proven ways of mitigating health risks associated with drug use and other high-risk behaviors may establish and operate a needle and hypodermic syringe access program. Provides objectives for programs established under the Act. Includes language requiring programs to provide specified services. Provides that no employee or volunteer of or participant in a program shall be charged with or prosecuted for possession of specified substances. Provides that law enforcement officers who in good faith arrest or charge a person entitled to immunity under the Act shall not be subject to civil liability for the arrest or filing of charges. Provides that prior to commencing operations under the Act, an organization shall report specified information to the Department of Public Health. Amends the Alcoholism and Other Drug Abuse and Dependency Act. Provides that the Department of Human Service shall give preference for grants and proposals to specified drug overdose prevention programs. Provides that the Department of Human Services shall conduct an evidence-based treatment needs assessment to be submitted to the General Assembly by December 31, 2019. Effective immediately. |
Passed both chambers |
|
HB0345
Same as SB0021 |
Lilly – Oak Park, D |
Amends the Prevention of Tobacco Use by Minors and Sale and Distribution of Tobacco Products Act. Changes the name of the Act to the Prevention of Tobacco Use by Persons under 21 Years of Age and Sale and Distribution of Tobacco Products Act. Raises the age for whom tobacco products, electronic cigarettes, and alternative nicotine products may be sold to and possessed by from at least 18 years of age to at least 21 years of age. Defines "electronic cigarette". Repeals the Smokeless Tobacco Limitation Act. Amends various other Acts to make conforming changes. Effective July 1, 2019. |
Public Act 101-0002 |
|
HB0465 |
Harris – Chicago, D |
Amends the Illinois Insurance Code. Provides that a contract between a health insurer and a pharmacy benefit manager must:(1) require the pharmacy benefit manager to update maximum allowable cost pricing information and maintain a process that will eliminate drugs from maximum allowable cost lists or modify drug prices to remain consistent with changes in pricing data; (2) prohibit the pharmacy benefit manager from limiting a pharmacist's ability to disclose the availability of a more affordable alternative drug; and (3) prohibit the pharmacy benefit manager from requiring an insured to make a payment for a prescription drug in an amount that exceeds the lesser of the applicable cost-sharing amount or the retail price of the drug. Contains provisions concerning the inclusion of prescription drugs on a maximum allowable cost list, State licensing requirements for pharmacy benefit managers, and other matters. Makes conforming changes to other Acts. Amends the Managed Care Reform and Patient Rights Act. Provides that a health care plan shall apply any third-party payments for prescription drugs. Makes changes to provisions concerning the denial of coverage for emergency services. Amends the Illinois Public Aid Code. Provides that the Department of Healthcare and Family Services may enter into a contract with any third party on a fee-for-service reimbursement model for the purpose of administering pharmacy benefits. Requires the Department to ensure coordination of care between the third-party administrator and managed care organizations as a consideration in any contracts established. Amends the Freedom of Information Act to exempt from disclosure certain information pharmacy benefits managers are required to provide under the Illinois Public Aid Code. Contains a severability provision. |
Passed in both Chambers |
|
HB0822 |
Halpin – Rock Island, D |
Amends the Care of Students with Diabetes Act. Provides that a school may maintain a supply of glucagon medication in any secure location that is accessible before, during, or after school where a student is most at risk, including, but not limited to, a classroom or the nurse's office; defines "glucagon medication" and "undesignated glucagon medication". Provides that a physician, a physician assistant who has prescriptive authority, or an advanced practice registered nurse who has prescriptive authority may prescribe undesignated glucagon medication in the name of the school to be maintained for use when necessary. Allows a delegated care aide to carry undesignated glucagon medication. Provides that within 24 hours after the administration of undesignated glucagon medication, a school must notify the school nurse and the student's parent or guardian or emergency contact, if known, and health care provider of its use. Effective immediately. |
Passed in both chambers |
|
HB0889 |
Swanson – Woodhull, R |
Amends the Illinois Insurance Code. Requires an individual or group policy of accident and health insurance or managed care plan to provide coverage for long-term antibiotic therapy for a person with a tick-borne disease. Makes conforming changes in the Health Maintenance Organization Act and the Illinois Public Aid Code. |
Passed in both chambers |
|
HB2160 |
Conroy – Villa Park, D |
Amends the Illinois Insurance Code. Requires the Department of Insurance to develop a uniform electronic prior authorization form to be used by an insurer that provides prescription drug benefits when requiring prior authorization. Provides that the development of the uniform electronic prior authorization form shall include input from specified interested parties and that the Department of Insurance shall take into consideration certain existing prior authorization forms and national standards pertaining to electronic authorization. Includes procedures for when a completed and accurate uniform electronic prior authorization form is not accepted by the insurer. Amends the Illinois Public Aid Code. Requires the Department of Healthcare and Family services to develop a uniform electronic prior authorization form to be used by a managed care organization that provides prescription drug benefits when requiring prior authorization. Provides that the development of the uniform electronic prior authorization form shall include input from specified interested parties and that the Department of Healthcare and Family Services shall take into consideration certain existing prior authorization forms and national standards pertaining to electronic authorization. Includes procedures for when a completed and accurate uniform electronic prior authorization form is not accepted by the managed care organization. |
Passed in both chambers |
|
HB2259 |
Feigenholtz – Chicago, D |
Amends the Medical Assistance Article of the Illinois Public Aid Code. Requires the Department of Healthcare and Family Services to develop, no later than January 1, 2020, a standardized format for all Medicaid managed care organization preferred drug lists in collaboration with Medicaid managed care organizations and other stakeholders, including, but not limited to, organizations that serve individuals impacted by HIV/AIDS or epilepsy, and community-based organizations, providers, and entities with expertise in drug formulary development. Requires the Department to allow Medicaid managed care organizations 6 months from the completion date of the standardized format to comply with the new Preferred Drug List format. Requires each Medicaid managed care organization to post its preferred drug list on its website without restricting access and to update the preferred drug list posted on its website no less than 30 days prior to the date upon which any update or change takes effect. Requires the Department to establish, no later than January 1, 2020, the Illinois Drug and Therapeutics Advisory Board to have the authority and responsibility to provide recommendations to the Department regarding which drug products to list on the Department's preferred drug list. Contains provisions concerning Board meetings and correspondence; the Board's composition; voting and non-voting members; and other matters. Requires the Department to adopt rules, to be in place no later than January 1, 2020, for the purpose of establishing and maintaining the Board. Effective immediately. |
Sent to Governor |
|
HB2896 |
Flowers – Chicago, D |
Amends the Department of Public Health Powers and Duties Law of the Civil Administrative Code of Illinois. Creates the Diversity in Health Care Professions Task Force. Provides that the Director of Public Health shall serve as the chairperson of the Task Force and it shall also be comprised of 2 dentists, 2 medical doctors, 2 nurses, 2 optometrists, 2 pharmacists, 2 physician assistants, 2 podiatrists, and 2 public health practitioners. Provides specified objectives. Provides specified recommendations to serve as guiding principals for the Task Force. Provides that Task Force members shall serve without compensation but may be reimbursed for their expenses incurred in performing their duties. Provides that the Task Force shall meet at least quarterly and at other times as called by the chairperson. Provides that the Department of Public Health shall provide administrative and other support to the Task Force. Provides that the Task Force shall prepare a report that summarizes its work and makes recommendations resulting from its study and shall submit the report of its findings and recommendations to the Governor and the General Assembly by December 1, 2020 and annually thereafter. |
Passed in both chambers |
|
HB3097 |
Mah – Chicago, D |
Amends the Illinois Public Aid Code. Requires the Department of Human Services to develop in collaboration with an academic institution a program designed to provide prescribing physicians under the medical assistance program with an evidence-based, non-commercial source of the latest objective information about pharmaceuticals. Provides that the prescriber education program shall consist of a web-based curriculum and an academic educator outreach and shall contract with clinical pharmacists to provide scheduled visits with prescribing physicians to update them on the latest research concerning medication usage and new updates on disease states in an unbiased manner. Provides that education provided under the prescriber education program shall include disease-based educational modules on the treatment of chronic non-cancer pain, diabetes, hypertension, and other specified diseases and that such modules shall be reviewed and updated on an annual or as-needed basis. Provides that additional resources provided under the prescribing education program shall include, but not be limited to: (i) a drug information response center available to prescribing physicians that provides thorough and timely in-depth answers to any questions a prescribing physician may have within 48 hours after a question is received; and (ii) information on drug utilization trends within individual and group practices. |
Passed in both chambers |
Marketing Affairs
Something Old, Something New, Something Borrowed, Something Blue - How Can Marketing Affairs Continue to Serve You?
by Bernice Man, PharmD, BCPS - ICHP Director of Marketing Affairs - Practice Coordinator, Specialty Pharmacy; Northwestern Medicine
Marketing Affairs has continued previously implemented initiatives such as promoting membership retention via contacting new members within three months of becoming an ICHP member and featuring two ICHP leaders in each KeePosted issue. We continued the annual Student Chapter Video Contest and this past year centered it around social media. Last but not least, our Champions project continues to move forward under Julie Downen’s excellent leadership. There are still a number of sites who do not have Champions, please contact Trish Wegner at trishw@ichpnet.org if you are interested in joining the Champion team!
One of our 2018-2019 goals is to increase ICHP’s social media presence. To this end, Melissa Dyrdahl, ICHP’s Communications Manager, created an infographic that outlines the various ways members can connect to ICHP and stay updated via Facebook, Twitter, Instagram, and LinkedIn. An initiative that has been ongoing and we hope to move forward through completion is obtaining the ICHP Board of Directors’ approval for a new network for technicians.
We are in the process of evaluating and leveraging ICHP’s website analytics information. To this end, we met with ASHP’s Director of Digital Marketing and Strategy and their Data Analyst in order to obtain guidance on how to best leverage ICHP’s online presence. ASHP provided extremely helpful information and we look forward to implementing these strategies in the upcoming year!
Something Blue
We identified that ICHPChat was not working out as a venue for membership discussion, so we are pivoting and in the process of moving that activity over to ICHP’s private Facebook group. Please join our Facebook group to participate in future discussions!
The inaugural year of my two-year term as ICHP’s Director of Marketing Affairs is quickly coming to a close. Many thanks to the dedicated members who participate in the Division of Marketing Affairs’ monthly conference calls. I look forward to how the group can move forward in 2020! Please do not hesitate to contact me with any new ideas for Marketing Affairs as we certainly want to tailor our activities to the needs of the ICHP membership!
1. Illinois Council of Health-System Pharmacists. Marketing Affairs Division. https://www.ichpnet.org/about_us/divisions_and_committees/display_division.php?division=division_of_marketing_affairs. 2019. Accessed June 25, 2019.
ICHP Leadership Spotlight Interview - Meet Brian!
Brian Cryder, PharmD, BCACP, CACP

Chair of the Ambulatory Care Network
Associate Professor, Midwestern University Chicago College of Pharmacy and Clinical Pharmacist, Advocate Medical Group (practicing at Beverly location).
My answer has evolved over time. I first chose pharmacy because of my experiences interacting with hospital pharmacists when I would volunteer at our community hospital growing up. They were always kind and willing to show how they mixed their IV medications (that I would then deliver to the nursing units) and reviewed the orders coming in from the physicians. I was fascinated by the work that they did; work that almost no patient even realized was happening behind the scenes. Later as a pharmacy student, I interned in the VA system and discovered how great it was to interact with patients and use what I had learned to improve their diabetes and other chronic conditions. This got me hooked on ambulatory care and has brought me to a place where seeing a patient improve really motivates me to do more for my patients and promote opportunities for other pharmacists to do the same. There are few greater things in life than to see that feeling of hope restored in a patient when they feel they can finally understand their medications and actually succeed in treating their chronic conditions that once seemed impossible.
Working through pre-conceived ideas that patients have. These problems range from patients who have a difficult time understanding why I am a pharmacist who does not actually dispense medication to impressions about certain medications patients hold onto from what they hear on television or from a neighbor. Educating patients about the role and proper use of their medications seems simple, but can be one of the most impactful interventions we can do as pharmacists. It is easy to fall in the trap of assuming they know what a medication is just because it has been prescribed for several years, but engaging with patients about all of the medication use details can identify pitfalls that prevent the best outcomes available to them.
ICHP is important because it provides an opportunity to connect with others in the profession to learn from each other and together advocate for the importance of the pharmacist’s role within the healthcare team.
I joined ICHP in 2003 upon joining the faculty at Midwestern University. Lynn Patton, who was at Midwestern at the time, was a strong advocate for getting involved in the state pharmacy organizations and recruited me as well as many other early career faculty to get involved with ICHP.
Virtually every person that I have worked with over my time as a student, intern, or pharmacist has influenced who I am as a pharmacist. If I had to highlight just a couple key influencers I would point to Dave Jansen and Debra Parker. Dave was the ambulatory care pharmacist at the Chillicothe, Ohio VA who really introduced me to ambulatory care and sparked my interest in the setting. Debra was my residency director at Physicians, Inc who really set the bar high by modeling how to be an impactful pharmacist through her interactions with patients, the physician team, students she precepted and other office staff – she expected a lot, but always held herself to that same standard.
Remember why you wanted to be a pharmacist in the first place. Virtually every prospective student that interviews for pharmacy school admission talks about how much they want to help others and make a difference for patients. Unfortunately, many times the pressures of completing pharmacy training can move your focus to the day to day tasks of assignments and achieving certain grades rather than keeping attention on the bigger picture of becoming a pharmacist that can make a difference for patients. I have never had a patient ask me what grade I received from any of my classes, but countless patients have asked “can you help me?”. While passing classes is important, if you aim first to learn what you need to know to be the best possible pharmacist in caring for your patients, the grades will be good enough to get you there.
I like a wide range of foods, so it is easier to list the foods I do not like – sushi and liver (could never bring myself to eat it after pharmacy school taught me that the liver is the “water treatment plant of the body”).
My family has a very strong medical orientation – my wife is a nurse practitioner, my brother is a physician assistant, my uncle is a family medicine physician, my mother and aunt are both nurses, an aunt was an occupational therapist, another aunt is a psychologist, a cousin is a physical therapist and another cousin is a veterinarian (for good measure). There is a running joke that we should start our own health center. Of those who are not medical, most are teachers, so with my faculty appointment I have that covered, too.
ICHP Leadership Spotlight Interview - Meet Andrew!
Andrew Merker, PharmD, BCPS, BCIDP, AAHIVP

Northern Illinois Society of Health-System Pharmacists - Secretary
Assistant Professor of Pharmacy Practice, Chicago College of Pharmacy, Internal Medicine Pharmacist, Mount Sinai Hospital
What our profession is going to look like in 10, 20, and 30 years from now. With increased automation and advanced technology, it’s important for pharmacists and technicians to continue to adapt and develop new methods of providing patient care. It is one reason why organizations like ICHP are important, to promote discussion and advancement of our profession. Although the future is unknown, I’m excited to
Recently at my practice site, I’ve been heavily involved in implementing a policy for guiding management of patients experiencing opioid withdrawal. There was no policy previously, which resulted in over utilization of methadone and in some instances, required naloxone administration to reverse side effects. In addition to policy creation, I helped lead provider/pharmacist/nurse education. As a result of this policy and education we have been more judicious with our methadone use by substituting buprenorphine (a safer alternative) and have future goals of increasing naloxone dispensing and medication assisted treatment (MAT) in our associated clinics.
ICHP is great because of the collaboration between pharmacists and technicians from diverse practice settings. I’ve enjoyed working with a variety of pharmacists and technicians and learning from their personal experiences while working to promote our profession. The discussion has allowed me to be more creative in my own problem solving skills.
I joined ICHP in late 2016 to assist in the planning for the 2017 Annual Meeting. I had been out of residency for a couple of years and was looking to get more involved with professional organizations on a regional/state level. I felt I had more experience to offer at that point in my career and I wanted to know the level of organization and planning that goes into such a large event. I had a great experience and learned a lot.
A special thanks to Bill Reay for making me who I am today in my career. During my junior year in college, I was considering pharmacy but was undecided. I was able to connect with Bill who shared his experiences and initiated a level of enthusiasm within me to pursue pharmacy. Throughout the years, he was always there to motivate me for the next step in my career. He connected me with several pharmacists who helped in my decision making process. Without his guidance, I’m sure my career path would have turned out extremely different.
The advice I always pass on to students is take advantage of opportunities presented and don’t be afraid to try something new. Some of my favorite and most beneficial opportunities came from offers I didn’t know I would enjoy initially. There is always something one can learn about themselves regardless if the opportunity fits in your “planned” career path or not.
Tacos have to be my favorite food. I find it hard to believe you can ever go wrong putting meat, cheese, and vegetables in a tortilla. They can be a part of any meal and I can eat them every day.
San Juan, Puerto Rico. It’s beautiful, lots of beaches, a quick flight from Chicago, and the food is amazing.
ICHPeople
 Great Job Dr. Janet Engle! Jan recently accepted the position of Executive Director at ACPE, where she will serve as the chief administrative officer for the organization. Jan starts her new job this September! Congrats Jan!
Great Job Dr. Janet Engle! Jan recently accepted the position of Executive Director at ACPE, where she will serve as the chief administrative officer for the organization. Jan starts her new job this September! Congrats Jan!  ICHP would like to extend our warmest congratulations to member, Dr. Henri Manasse! Dr. Manasse, a respected educator and leader in our industry, was recently awarded the "ASHP Board of Directors' Honorary Membership Award". He also received ICHP honorary membership in 2013. Thank you Henri for all the contributions you've made and continue to make to pharmacy practice!
ICHP would like to extend our warmest congratulations to member, Dr. Henri Manasse! Dr. Manasse, a respected educator and leader in our industry, was recently awarded the "ASHP Board of Directors' Honorary Membership Award". He also received ICHP honorary membership in 2013. Thank you Henri for all the contributions you've made and continue to make to pharmacy practice! 


Educational Affairs
Angiotensin Receptor Blocker Recalls: What Did We Learn?
by Tomasz Jurga, PharmD - Assistant Professor of Clinical Sciences, Roosevelt University College of Pharmacy
- Limited evidence of carcinogenicity in humans
- Sufficient evidence of carcinogenicity in experimental animals
- Strong evidence that the agent exhibits key characteristics of carcinogens
Table 1. The International Agency for Research on Cancer (IARC) Carcinogenic Classifications |
|
|
Classification |
Definition |
|
Group 1 |
Carcinogenic to humans |
|
Group 2A |
Probably carcinogenic to humans |
|
Group 2B |
Possibly carcinogenic to humans |
|
Group 3 |
Not classifiable as to its carcinogenicity to humans |
|
Group 4 |
Probably not carcinogenic to humans |
- During this period of drug recall and limited availability, pharmacists can do the following:
- Focus on proper patient education - With the new FDA statement requiring better impurity testing techniques, the next drug recall is likely unavoidable. Be prepared to answer questions from patients and providers and understand the background and reasons for the recall. Focus on proper prescriber education - Pharmacists should inform physicians not to discontinue medications without checking to see if other manufacturers are available. Switching medications that have not been affected can be counterproductive. It can increase workload for pharmacists who are already working on replacing affected drugs. This can in turn lead to increased wait times and even more patient dissatisfaction.
- Take an active role in replacing affected medications – Aim for minimal interruption to a patient’s medication regimen. Some hospital pharmacies have released specific instructions for lot substitutions. They have also notified healthcare workers about the lot and manufacturer changes. In many cases, hospital pharmacies have switched from an affected ARB to an unaffected one without interrupting patients’ therapies. Community pharmacists reached out to patients to notify them if their medications have been affected. Ambulatory care pharmacists should educate patients and prescribers about the nature of the recall to prevent unnecessary adjustments at the prescriber level.
- Check the FDA recall list to see when/if new recalls are announced: https://www.fda.gov/Safety/Recalls/default.htm Check the FDA ARB recall list for specific information on ARBs: https://www.fda.gov/drugs/drug-safety-and-availability/fda-updates-and-press-announcements-angiotensin-ii-receptor-blocker-arb-recalls-valsartan-losartan
- Consider the whole picture. When answering questions about possible dangers and risks, remember to focus on life-time exposure and weigh the benefits-risks for each patient.
References:
1. Food and Drug Administration. Major Pharmaceuticals Issues Voluntary Nationwide Recall of Valsartan Due to The Potential Presence of a Probable Carcinogen (NDMA) (July 2018). www.fda.gov/Safety/Recalls/ucm613625.htm (accessed 2019 Jan 31).
2. Sipahi I, Debanne SM, Rowland DY, Simon DI, Fang JC. Angiotensin-receptor blockade and risk of cancer: meta-analysis of randomised controlled trials. Lancet Oncol. 2010;11(7):627-636.
3. Angiotensin receptor blockers linked to “modest” increase in cancer risk, Lancet study reveals. The Pharmaceutical Journal. 2010;284:602.
4. Chiang YY, Chen KB, Tsai TH, Tsai WC. Lowered cancer risk with ACE inhibitors/ARBs: a population-based cohort study. J Clin Hypertens (Greenwich). 2014;16(1):27-33.
5.
Food and Drug Administration. FDA
updates on angiotensin II receptor blocker (ARB) recalls including valsartan,
losartan and irbesartan (June 2019).
fda.gov/drugs/drug-safety-and-availability/fda-updates-and-press-announcements-angiotensin-ii-receptor-blocker-arb-recalls-valsartan-losartan
(accessed 2019 June 19).
6.
Citizen Petition from Valisure, LLC (June 2019).
regulations.gov/document?D=FDA-2019-P-2869-0001 (accessed 2019 June 19).
7.
World Health Organization. International Agency
for Research on Cancer. IARC Monographs on the Identification of Carcinogenic
Hazards to Humans Preamble (2019).
monographs.iarc.fr/wp-content/uploads/2019/01/Preamble-2019.pdf
(accessed 2019 Jan 31).
8.
World Health Organization. International Agency
for Research on Cancer. Agents Classified by the IARC
Monographs, Volumes 1-123 (2018).
monographs.iarc.fr/wp-content/uploads/2018/09/List_of_Classifications.pdf (accessed
2019 Jan
31).
9. N-Nitrosodiethylamine. Pubchem Open Chemistry Database. US National Library of Medicine. pubchem.ncbi.nlm.nih.gov/compound/5921 (accessed 2019 Jan 31).
10.
N-Nitrosodimethylamine. Pubchem Open Chemistry
Database. US National Library of Medicine.
pubchem.ncbi.nlm.nih.gov/compound/6124 (accessed 2019 Jan 31).
11.
N-Methyl-N-(3-carboxypropyl)nitrosamine.
Pubchem Open Chemistry Database. US National Library of Medicine.
pubchem.ncbi.nlm.nih.gov/compound/N-Methyl-N-_3-carboxypropyl_nitrosamine (accessed
2019 June 19).
12. Liteplo RG, Meek ME, Windle WE. Concise International Chemical Assessment Document 38: N-Nitrosodimethylamine. World Health Organization. 2002.
13. US Food and Drug Administration (FDA). M7(R1) Assessment and Control of DNA Reactive (Mutagenic) Impurities in Pharmaceuticals To Limit Potential Carcinogenic Risk Guidance for Industry (March 2018). www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM347725.pdf (accessed 2019 Jan 31).
14. Food and Drug Administration. Statement from FDA Commissioner Scott Gottlieb, M.D., and Janet Woodcock, M.D., director of the Center for Drug Evaluation and Research on the FDA’s ongoing investigation into valsartan and ARB class impurities and the agency’s steps to address the root causes of the safety issues (January 2019). www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm629796.htm (accessed 2019 Jan 31).
15. Brenner BM, Cooper ME, de Zeeuw D, et al. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med. 2001;345:861-869
16. Pitt B, Poole-Wilson PA, Segal R, et al. Effect of losartan compared with captopril on mortality in patients with symptomatic heart failure: randomised trial - the Losartan Heart Failure Survival Study, ELITE II. Lancet. 2000;355:1582–1587
17. Potegard A, Kristensen KB, Ernst MT, Johanses NB, Quartarolo P, Hallas J. Use of N-nitrosodimethylamine (NDMA) contaminated valsartan products and risk of cancer: Danish nationwide cohort study. BMJ. 2018;362:k3851.
Educational Affairs
Call for Posters!
Please consider sharing the outcomes with your colleagues at the poster session during the ICHP Spring Meeting March 27-28, 2020 in East Peoria, IL! This is a great opportunity to share innovative ideas with others and learn about trends in Illinois health-system pharmacies.
All ICHP members are eligible to submit abstracts to be considered for presentation at the Spring Meeting. For more information on categories for submission, platform presentations and eligibility criteria, please visit our website.
Members wishing to submit a poster should use the online submission form. Be sure to click "Submit" after completing your form. The deadline for submissions is January 10, 2020. Please direct any questions to Trish Wegner at TrishW@ichpnet.org.
Submission deadline is January 10, 2020. Authors will be notified of acceptance of their poster via email in February, 2020.
Professional Affairs
Pharmacist's Role in Suicide Awareness and Prevention
by Jen Phillips, PharmD, BCPS, FCCP, FASHP Associate Professor - Midwestern University; Clinical Pharmacist - AdvocateAuroraHealth; Maggie Lau, PharmD PGY-1 Resident VA San Diego Healthcare System
- Suicide is not proactively identified. Data suggest that more than half of patients who succumb to suicide had a healthcare visit within the month preceding their death. There may be a perception among healthcare providers that only mental health specialists have the training and responsibility to manage patients at risk for suicide. Others may be afraid to broach the subject, fearing that talking about it may “plant the idea” in the patient’s head. Both of these thought processes are unfounded. Healthcare professionals need to feel comfortable assessing risk for suicidality in patients. Educational programming is needed, along with the development and use of effective screening tools that are feasible to incorporate into practice.8
- Lack of effective action. Currently, most patients who present with suicidal thoughts are either hospitalized for a short period or referred to a mental health specialist. The National Alliance suggests that both of these options are not enough. A short-term hospitalization may not be long enough to reduce suicide risk. In addition, it may take a while for a patient to get an outpatient appointment and suicide risk is highest in the time immediately following hospitalization. The National Alliance suggests an alternative option where healthcare providers work with the patient to develop a “safety plan” including identifying triggers and using methods to manage thoughts and impulses safely. Additionally, providers should work with the patient to reduce immediate access to lethal means.8
- Lack of supportive contact. It is important for healthcare providers to follow-up with patients who express suicidal thoughts after discharge. This may be in the form of telephone calls, messages, or follow-up visits. This helps remove the feeling of isolation that may precipitate suicidality by reinforcing to the patient that there is a caring contact available to them.8
References
- World Health Organization. Suicide Data. http://www.who.int/mental_health/prevention/suicide/suicideprevent/en/. Accessed 2018 September 23.
- Centers for Disease Control and Prevention. Suicide Rates Rising Across the US. https://www.cdc.gov/vitalsigns/suicide/index.html. Accessed 2018 September 23.
- American Foundation for Suicide Prevention. Suicide Statistics. https://afsp.org/about-suicide/suicide-statistics/. Accessed 2018 September 23.
- Centers for Disease Control and Prevention. Web-based Injury Statistics Query and Reporting System (WISQARS). https://www.cdc.gov/injury/wisqars/index.html. Accessed 2018 September 23.
- Substance Abuse and Mental Health Services Administration. (2017). Key Substance Use and Mental Health Indicators in the United States: Results from the 2016 National Survey on Drug Use and Health (HHS Publication No. SMA 17-5044, NSDUH Series H-52). Rockville, MD: Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. https://www.samhsa.gov/data/sites/default/files/NSDUH-FFR1-2016/NSDUH-FFR1-2016.htm.
- Centers for Disease Control and Prevention. Suicide: Risk and Protective Factors. https://www.cdc.gov/violenceprevention/suicide/riskprotectivefactors.html. Accessed 2018 November 20.
- The Joint Commission. Detecting and treating suicide ideation in all settings. Sentinel Event Alert. 2016 56(3).
- National Action Alliance for Suicide Prevention: Transforming Health Systems Initiative Work Group (2018). Recommended standard care for people with suicide risk: Making health care suicide safe. Washington, Dc: Education Development Center, Inc.
- Lavigne. Suicidal ideation and behavior as adverse events of prescribed medications: An update for pharmacists. J Am Pharm Assoc. 2016;56:203-6.
- American Society of Health-System Pharmacists. Joint council recommendation: suicide awareness and prevention. https://connect.ashp.org/communities/ (accessed 2019 May 14).
New Practitioners Network
Making the Most of Mentorship: Advice for how to Maintain a Mentor Relationship
by Abby Lodico, PharmD, PGY-1 Pharmacy Resident, Northwestern Medicine, Chicago, IL; W. Justin Moore, PharmD, PGY-1 Pharmacy Resident, Northwestern Medicine, Chicago, IL
Features
Make Your Plans -
Pharmacy Month, Week and Day are Approaching!
by Scott A. Meyers, Executive Vice President
Collaborative Pharmaceutical Task Force Report - June
Recommendations Finally Get a Vote!
by Scott A. Meyers, Executive Vice President
Motion regarding “Pharmacy Technician on Duty”
- “requiring pharmacies to have at least one pharmacy technician on duty whenever the practice of pharmacy is conducted.”
Motion No. 2
Motion regarding “Triple Pay for No Breaks”
- “to pay the pharmacist 3 times the pharmacist’s regular hourly rate of pay for each workday during which the required breaks were not provided.”
Motion regarding “Break Room”
- “to make available at all times a room on the pharmacy’s premises with adequate seating and tables for the purpose of allowing a pharmacist to enjoy break periods in a clean and comfortable environment.”
Motion No. 4
Motion regarding “Prescription Limits” and ”Pharmacy Technician Hours”
- “to set a prescription limit of not more than 10 prescriptions filled per hour;” and
- “to mandate at least 10 pharmacy technician hours per 100 prescriptions filled,”
(2) Failure to provide a working environment for all pharmacy personnel that protects that health, safety and welfare of a patient which includes, but is not limited to: . . . .(c) Adequate time for a pharmacist to complete professional duties and responsibilities including, but not limited to:(A) Drug Utilization Review;(B) Immunization;(C) Counseling;(D) Verification of the accuracy of a prescription; and
(E) All other duties and responsibilities of a pharmacist as specified in the Pharmacy Practice Act Administrative Rules Part 1300.
Motion regarding “Prohibiting Distractions”
- “to place a general prohibition on activities that distract pharmacists,”
(2) Failure to provide a working environment for all pharmacy personnel that protects that health, safety and welfare of a patient which includes, but is not limited to:
(a) Sufficient personnel to prevent fatigue, distraction or other conditions that interfere with a pharmacist’s ability to practice with competency and safety or creates an environment that jeopardizes patient care.
Motion No. 6
Motion regarding “No Work During Break”
- “to not require a pharmacist to work during a break period,”
(2) Failure to provide a working environment for all pharmacy personnel that protects that health, safety and welfare of a patient which includes, but is not limited to: . . .(b) Appropriate opportunities for uninterrupted rest periods and meal breaks
Motion regarding “Whistleblower Protection”
- “the extent to which providing whistleblower protections for pharmacists and pharmacy technicians reporting violations or worker policies,”
(5) Anyone reporting violations of this section to the Department of Financial and Professional Regulation are specifically protected under the Illinois Whistleblower Act” (740 ILCS 174/15(b)).
Motion No. 8A
Motion regarding “Length of Work Day”
- “to limit a pharmacist from working more than 8 hours a workday,”
A pharmacy licensed under Illinois Statutes, which is located within Illinois, shall not require a pharmacist, student pharmacist, or pharmacy technician to work longer than eight (8) continuous hours per day, inclusive of the breaks required under subpart 2.
Motion regarding “Length of Work Day”
- “to limit a pharmacist from working more than 8 hours a workday,”
A pharmacy licensed under Illinois Statutes, which is located within Illinois, shall not require a pharmacist, student pharmacist, or pharmacy technician to work longer than twelve (12) continuous hours per day, inclusive of the breaks required under subpart 2.
Motion No. 9
Motion regarding “Break Records”
- “to keep a complete and accurate record of the break periods of its pharmacists,”
The Employer shall keep and maintain a complete and accurate record of the daily break periods of its pharmacists.
Motion No. 10A
Motion regarding “Mandatory Breaks and Lunch Period”
- “to provide a pharmacist a minimum of 2 15-minute paid rest breaks and one 30-minute meal period in each working day on which the pharmacist works at least 7 hours,”
A. A pharmacist working longer than six continuous hours per day shall be allowed during that time period to take a 30-minute uninterrupted meal break and (2) 15-minute breaks. No pharmacist shall be required to work longer than 5 continuous hours per day without the opportunity to take an uninterrupted meal break.
Motion regarding “Mandatory Breaks and Lunch Period”
- “to provide a pharmacist a minimum of 2 15-minute paid rest breaks and one 30-minute meal period in each working day on which the pharmacist works at least 7 hours,”
A. A pharmacist working longer than six continuous hours per day shall be allowed during that time period to take a 30-minute uninterrupted meal break and (1) 15-minute break.
The pharmacist qualifies for an additional 15-minute break if working 12 continuous hours per day. No pharmacist shall be required to work longer than 5 continuous hours per day without the opportunity to take an uninterrupted meal break.
The Task Force concluded with a final review of proposed changes to the Practice Act and Rules related to pharmacy technician tasks and responsibilities. What is expected to be the final language recommended by the Task Force to the Department at the July meeting can also be found on the ICHP website. ICHP members should have already received an e-mail blast regarding this language and the Grounds for Discipline and Pharmacy Work Conditions documents in June. (Note: If you did not receive that important e-mail blast please ask your IT Department to whitelist www.ichpnet.org and look in your spam or junk folders to see if it landed there!)
Collaborative Pharmaceutical Task Force Report - July
More Recommendations Get a Vote!
by Scott A. Meyers, Executive Vice President
Motion regarding “Pharmacy Technician Continuing Education and Duties”
- In developing standards related to its discussions, the Collaborative Pharmaceutical Task Force shall consider the extent to which Public Act 99473 (enhancing continuing education requirements for pharmacy technicians) may be relevant to the issues listed in Section 4.5 of the Pharmacy Practice Act.
A. Require that pharmacy technicians be specifically trained for the tasks which they are assigned to accomplish, while retaining the exception that certain tasks cannot be delegated to pharmacy technicians;B. Require that pharmacy technicians obtain documentation from a pharmacist-in-charge verifying that he or she has successfully completed a standardized nationally accredited education and training program with an objective assessment mechanism to be licensed, if they have not graduated from a pharmacy technician training program meeting the requirements of the Ac t;C. Permit pharmacy technicians to administer vaccinations/immunizations to persons, as long as they successfully complete a course of training on the administration of vaccines approved by the Department and are directly supervised by a pharmacist; and
D. Permits student pharmacists and registered pharmacy technicians to transfer prescriptions between pharmacies for the purpose of original or refill dispensing, and to receive prescriptions for controlled substances from an employee or agent of the individual practitioner pursuant to the directions and order of that practitioner.
Motion regarding “Pharmacy Prescription Systems Contain Mechanisms that Require Prescription Discontinuation Orders to be Forwarded to a Pharmacy”
- [T]he extent to which requiring the Department to adopt rules requiring pharmacy prescription systems contain mechanisms to require prescription discontinuation orders to be forwarded to a pharmacy.
A. Effective January 1, 2021, all pharmacies that use the SCRIPT standard for receiving electronic prescriptions must enable, activate, and maintain the ability to receive transmissions of electronic prescription cancellation and to transmit cancellation response transactions.
B. Within two (2) business days of receipt of a prescription cancellation transaction, pharmacy staff must either review the cancellation transaction for deactivation or provide that deactivation occurs automatically.
Motion regarding “Pharmacy Employee Termination”
- In developing standards related to its discussions, the Collaborative Pharmaceutical Task Force shall consider the extent to which Public Act 99-863 (enhancing reporting requirements to the Department of pharmacy employee terminations) may be relevant to the issues listed in paragraphs (1) and (2).
PTCB'S Recertification Process is Now Easier and Faster
CPhTs Need to have an NABP E-Profile ID Before Recertifying
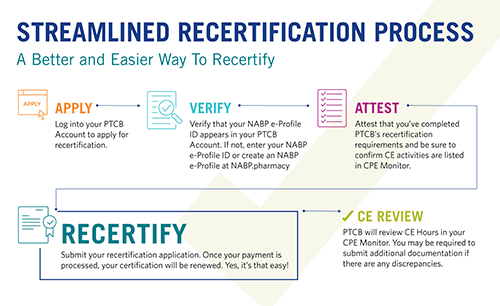
- Eliminates the need to manually enter CE information already entered into CPE Monitor
- Provides instant recertification/reinstatement
- Quick and efficient application
To set up an NABP e-Profile, CPhTs visit NABP’s website and create one. After creating their e-Profile account, they must be sure to add their PTCB Certification Number to the Credentials section of their NABP e-Profile. CPhTs should ensure that their e-Profile ID and birth date (month and day) match in their PTCB Account and NABP e-Profile. To update their birth date in their NABP e-Profile, they can follow these instructions.
After logging into their PTCB Account, they look for the check mark next to their e-Profile ID on their Account home page. If they do not see the check mark, they can add their e-Profile ID by clicking ‘Add your e-Profile’ under ‘Profile Summary’ or when applying for renewal.
In coordination with this upgrade, PTCB will adjust the recertification fee for the first time in more than a decade (since 2007). Beginning October 2, 2019, the recertification fee will be $49 and the reinstatement fee will be $89. The existing $25 Late Application Processing Fee and $10 Reprocessing Fee will not change.
We Need Your Feedback!
Join us for the 2019 ICHP Annual Meeting
Impact Patient Care

College Connection
Midwestern University Chicago College of Pharmacy
Discovering Serendipity: Reflections of a Third-Year Pharmacy Student
College Connection
by Honey Joseph, PS3, ICHP Membership Chair Midwestern University Chicago College of Pharmacy
Roosevelt University College of Pharmacy
Meet the New E-Board and why we Chose to be a Part of ICHP-SSHP
College Connection
by Jeremy Fernandez Balingit, PS-2, SSHP President Roosevelt University College of Pharmacy
President - Jeremy Fernandez Balingit
Vice President - Priya Patel
Treasurer - Adeola Lawal
Secretary - Swetha Sajan

Rosalind Franklin University College of Pharmacy
Interprofessional Health Screening Events at RFU
College Connection
by Rita Piro, PS-3, ICHP Vice President Rosalind Franklin University of Medicine and Science College of Pharmacy
Southern Illinois University Edwardsville School of Pharmacy
Meet the Executive Board
College Connection
by Justin Shiau, P2, President-Elect SIUE School of Pharmacy
University of Illinois at Chicago College of Pharmacy
"It's OK not to be OK" De-Stigmatizing Conversations Surrounding our Mental Health
College Connection
by Josiah Baker, P3, PharmD Candidate, ICHP Student Chapter President University of Illinois at Chicago College of Pharmacy

More
Welcome New Members!
Arti Aravindan - Recruited by Alexis Tandyk
Maureen Barnes-Israel
Natasha Brown - Recruited by Richard Puccetti
Sara Brown - Recruited by Kathryn Schultz
Heather Bryant - Recruited by Travis Hunderdosse
Brittany Crawford - Recruited by Richard Puccetti
Jeremy Fernandez Balingit - Recruited by Sara Koehnke
Emily Forbes
Lidiane Gabeira
Alex Holub
Jessica Jones - Recruited by David Huhtelin
Alicia Jones
Dagmara Kutrzuba - Recruited by Alexis Tandyk
Renee McTee
Farrah Naama
Ishmael Ochir - Recruited by Richard Puccetti
Daniel Osei-Bonsu
Allison Rodawold
Jazmine Rosales
Ruba Samara
Kasia Szaflarska - Recruited by Alexis Tandyk
Darlisa Taylor - Recruited by Richard Puccetti
Danny Tran
Malgorzata Labedz
Rachel Nass - Recruited by Ann Jankiewicz
Michael Gabay
Jon O'Connor
Jan Powell
Sadaf Suleman
Panagiota Terzis
Syed Ahmed
Matthew Allsbrook - Recruited by Travis Hunerdosse
Ana Alvarado
Chinchumol Baby
Jessica Banks
Maria Barrios
Cynthia Bautista
Amanda Bentley - Recruited by Amy Boblitt
Lindsey Blomgren - Recruited by Levi Youngs
Emily Boyer - Recruited by Madison Fleckenstein
Johnathan Brooks
Sophia Brown
Jessica Carlson
Nicholas Cirone
Allison Cowett - Recruited by Lara Ellinger
Nahreen Dammo
John Davis
Paris Dotson
Thorsten Ericksen
Anna Flores
Catherine Floyd
April Frischkorn - Recruited by Tonya Roley
Lucia Garcia
Glen Gard - Recruited by Scott Meyers
Alex Goneh
Ancy John
Chinchu Perumbel John
Heather Khali - Recruited by Kristi Stice
Sarah Lee
Brooke Lowe - Recruited by Lisa Ingram
Jennifer Miller
Ommar Mohammed - Recruited by Nour Shaban
Rohy Ortiz
Bhavna Patel
Helly Patel
Nisha Patel
Cathleen Perez
Franklin Ponce - Recruited by Ellen Smith
Portsha Sample - Recruited by Antoinette Cintron
Barry Sealy
Nour Shaban
Gautam Shah
Jessica Sheridan
Jade Sproles
Freddy Tadros
John Ullery
April West - Recruited by Kara Ozee
Barbara White
Renee Youmara
ICHP Pharmacy Action Fund
Contributors
.jpg)
Upcoming Events
August 13, 2019
Topic: Put the "Live" Back into Liver: Management of Decompensated Liver Disease
Speaker: Carrie Vogler, PharmD, BCPS
Accredited for Health-System Pharmacists
August 13, 2019
Chicago, IL & Springfield, IL
August 14, 2019 - Noon
Topic: IBD: Biologic Therapeutic Drug Monitoring
Speaker: David Choi, PharmD, BCACP
Accredited for Health-System Pharmacists
See your practice site Champion to participate!
September 12-14, 2019
Drury Lane Conference Center - Oakbrook Terrace, IL
October 16, 2019
Park Ridge Country Club - Park Ridge, IL
SAVE THE DATE - More information to follow.
November 15-16, 2019
I Hotel and Conference Center - Champaign, IL
By invitation only
November 21, 2019
RPM Italian, Chicago, IL
SAVE THE DATE - More information to follow.
2020 ICHP SPRING MEETING
March 27-28, 2020
Embassy Suites Conference Center - East Peoria, IL
Educational Affairs: 3rd Tuesday of each month - 11:00 am
Executive Committee: 2nd Tuesday of each month - 7:00 pm
Government Affairs: 3rd Monday of each month - 5:00 pm
Marketing Affairs: 3rd Tuesday of each month - 8:00 am
Organizational Affairs: 2nd Wednesday of each month - 3:00 pm
Professional Affairs: 4th Tuesday of each month - 3:00 pm
Technology Committee: 2nd Friday of each month - 8:00 am
Regularly Scheduled network meetings
340B NETWORK: See ICHP calendar for details
Ambulatory Care Network: 1st Thursday each month - 12:00 pm
Chicago area pharmacy directors network dinner meeting: See ICHP calendar for details
New Practitioners Network: 3rd Tuesday of each month - 5:30 pm
Small and Rural Hospitals: See ICHP calendar for details
Board of Directors
2018-2019
120x120.jpg) Noelle Chapman
President
|
 Travis Hunerdosse
Immediate Past President,
Committee Chair, Nominations Committee
|
 Carrie Vogler
President-Elect
217-545-5394
|
 Kathryn Schultz
Treasurer
|
 Ed Rainville
Secretary
|
 Scott Meyers
Executive Vice President ICHP Office
|
 Amy Boblitt
Regional Director Central
|
 Elise Wozniak
Regional Director Northern
|
 Lynn Fromm
Regional Director Southern
|
 Mary Lee
Organizational Affairs Director
|
 Karin Terry
Professional Affairs Director
|
 David Martin
Educational Affairs Director
|
 Bernice Man
Marketing Affairs Director
|
 Christopher Crank
Government Affairs Director
|
 Kristine VanKuiKen
Technician Representative
|
 Bryan McCarthy
Chairman, New Practitioners Network
|
 Brian Cryder
Ambulatory Care Network Chair
|
 David Tjhio
Chairman, Committee on Technology
|
 125x125 for KP digital.jpg) Jennifer Phillips
Editor & Chairman - KeePosted
|
 Milena McLaughlin
Assistant Editor - KeePosted
|
 Sandra Durley
340B Network Chair |
 Tara Vickery Gorden
Small and Rural Hospital Network Chair |
Sanad Abduljawad
Chicago State University College of Pharmacy
|
Irum Khan
Midwestern University Chicago College of Pharmacy
|
Jeremy Fernandez Balingit
Roosevelt University College of Pharmacy
|
Nimita Shah
Rosalind Franklin University College of Pharmacy
|
Kristen Ingold
Southern Illinois University Edwardsville School of Pharmacy
|
Josiah Baker
University of Illinois at Chicago College of Pharmacy
|
Bill Clafshenkel
University of Illinois at Chicago, Rockford Campus, College of Pharmacy
|
Denise Kolanczyk
President
|
Milena McLaughlin
President-elect
|
Erika Hellenbart
Immediate Past President
|
David Martin
Treasurer
|
Andrew Merker
Secretary
|
Richard Puccetti
Technician Representative
|
Ed Rainville
President
|
Jared Sheley
President
|
Billee Samples
President
|
Megan Stoller
President-elect
|
Julie Downen
Immediate Past President
|
President - Rock Valley Society
|
President - Southern IL Society
|
President - Sugar Creek Society
|