Official Newsjournal of the Illinois Council of Health-System Pharmacists

Educational Affairs
New Oncology Drugs of 2017: Novel Intravenous Approvals
by Christopher Campbell, PharmD, BCPS, BCOP, Northwestern Memorial Hospital; Janna Afanasjeva, PharmD, BCPS, Northwestern Memorial Hospital; Chloe Majkowski, PharmD Candidate 2018, University of Illinois Chicago
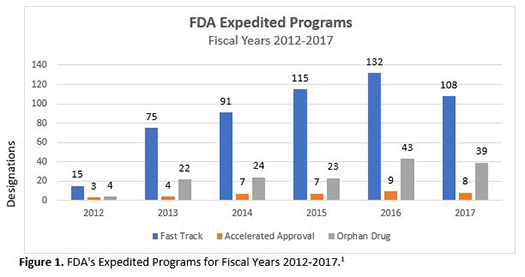
With major advances in science and technology over the past few decades, the pharmaceutical industry has discovered better drug targets and applied this to drug development. Simultaneously, the Food and Drug Administration (FDA) introduced fast track, breakthrough therapy, and priority review designations, along with accelerated approval pathways, which have allowed new medications for treating serious conditions to reach the market much sooner than ever before. As Figure 1 demonstrates, expedited approvals for fast track, orphan drug, and accelerated approvals have increased to approximately 100, 40, and 10 respective designations or approvals per year.1 In 2017, 12 of 46 (26%) total novel drug approvals were in hematology and oncology alone, including 9 new molecular entities and 7 new monoclonal antibodies.2-4 The year 2017 also saw biologics license applications (BLAs) approved for the first 2 chimeric antigen receptor (CAR) T-Cell therapies, axicabtagene ciloleucel and tisagenlecleucel. These therapies are completely new methods of gene therapy utilizing modified versions of the patient’s own immune system to attack certain cancers in the blood. The purpose of this article is to provide a brief overview of the intravenous drug approvals in oncology for year 2017 that showcase innovation and the great strides being accomplished in treating cancer. Drug reviews include information on indications, special designations, efficacy, safety, and place in guidelines. Table 1 provides additional information on dosage forms, administration, and cost.
Avelumab (Bavencio®)
Indication
Avelumab received accelerated approval for metastatic Merkel cell carcinoma (MCC) in adult and pediatric patients 12 years of age and older and for locally advanced or metastatic urothelial carcinoma (UC) in patients who have progressed on or after a platinum-containing chemotherapy regimen.5 The MCC indication had priority review, breakthrough therapy, and orphan drug status, as avelumab was the first FDA approved treatment for this disease. Urothelial carcinoma, a difficult to treat tumor, was given priority review.6,7 Avelumab inhibits programmed death-ligand 1 (PD-L1) receptor located on tumor cells, blocking the inhibition of T-cells and restoring immune response to tumor cells. Avelumab also engages the innate immune system and induces antibody-dependent cell-mediated cytotoxicity (ADCC).
Efficacy
The accelerated approvals of avelumab were based on 2 clinical trials: JAVELIN Merkel 200 and the UC cohort of the JAVELIN Solid Tumor trial.5 JAVELIN Merkel 200 was an open-label phase 2 study of avelumab monotherapy (10 mg/kg IV every 2 weeks) in 88 patients with metastatic MCC, who had prior chemotherapy.5,8 At the time of publication, the primary endpoint, the objective response rate (ORR), was 31.8% (95% confidence interval [CI], 21.9% to 43.1%) with 8 (9%) complete responses (CR) and 20 (23%) partial responses. Median progression-free survival (PFS) was 2.7 months, and median overall survival (OS) was 11.3 months. Results after 1 year follow-up included an updated ORR of 33%, due to 2 additional patients achieving a CR. The duration of response (DOR) in 29 patients was 86% over 6 months and 45% over 12 months. Responses were independent of PD-L1 tumor expression.
JAVELIN Solid Tumor was an open-label, single-arm, large phase 1b study of avelumab (10 mg/kg IV every 2 weeks) with a pooled analysis of 2 cohorts consisting of 241 patients with metastatic UC, in whom 95.4% had progressed on platinum-based therapy.5,9 At the time of abstract publication, there was a demonstrated primary endpoint ORR of 17.6% (95% CI, 12.0 to 24.6) in 27 out of 153 patients with at least 6 months follow-up. Median PFS was 6.4 weeks (95% CI, 6.1 to 11.4); however, median DOR was not reached. At the time of the FDA approval, ORR response dropped to 13.3%, and a median DOR had still not been reached (range in months of 1.4+ to 17.4+).5
Safety
In the JAVELIN Merkel 200 study, the most common adverse reactions reported were fatigue (50%), muscle pain (32%), diarrhea (23%), nausea (22%), infusion-related reaction (22%), rash (22%), decreased appetite (20%), and peripheral edema (20%).5 Immune-related adverse reactions included treatment-emergent abnormalities such as grade 3 to 4 elevated liver enzymes, increased bilirubin, and creatinine kinase elevation. Anemia was the most common reason for dose interruption. Permanent discontinuation was required for ileus, nephritis, transaminitis, and pericardial effusion. The UC cohort of the JAVELIN Solid Tumor trial also reported common infusion-related reactions (22.8%) and fatigue (12.0%).9 According to the published abstract, Grade 3 to 4 immune-related adverse reactions occurred in 11.6% of patients including 1 treatment-related death due to pneumonitis. However, the package insert describes that 14 patients (6%) from the pooled cohort died due to pneumonitis, respiratory failure, sepsis, cerebrovascular accident, or gastrointestinal adverse events.5
Guidelines
The NCCN Bladder Cancer guideline recommends avelumab in UC as a second-line single agent systemic therapy option for locally advanced or metastatic disease.10 The NCCN MCC guideline recommends avelumab for disseminated clinical M1 disease with or without surgery and/or radiation therapy.11
Axicabtagene ciloleucel (Yescarta™)
Indication
Axicabtagene ciloleucel is approved for use in adults with relapsed or refractory (r/r) B-cell lymphoma, such as diffuse large B-cell lymphoma (DLBCL) and other high grade lymphomas after fludarabine and cyclophosphamide lymphodepleting chemotherapy.12,13 Axicabtagene ciloleucel has not been studied in patients with primary central nervous system lymphoma and is not indicated for this population. The FDA granted priority review and orphan drug status to axicabtagene ciloleucel for this indication. Axicabtagene ciloleucel is the first treatment for B-cell lymphoma that targets CD19-expressing malignant cells with genetically modified autologous T-cells encoded with a CAR. Binding of CAR T-cells to CD19 activates a T-cell signaling cascade leading to the activation, proliferation, secretion of inflammatory cytokines, and ultimately to elimination of CD19 target cells.
Efficacy
Axicabtagene ciloleucel was approved for r/r B-cell lymphoma based on results from the ZUMA-1 trial.12 The ZUMA-1 trial was an open-label, phase 2, multicenter, single-arm trial assessing the safety and efficacy of a single infusion of axicabtagene ciloleucel therapy in 111 patients enrolled (101 treated) with r/r B-cell non-Hodgkin lymphomas (NHLs), primarily DLBCL.14 Patients with an Eastern Cooperative Oncology Group (ECOG) performance status of 0 to1 were included, and 77% of the patients had refractory disease to 2 or more lines of therapy including autologous stem cell transplant.15 The primary endpoint was an investigator-assessed ORR of 82% with ongoing responses in 44% of patients at 8.7 months.14 Tocilizumab and/or steroid use did not impact ORR. The median PFS was 5.9 months (95% CI, 3.4 to 9.8), while median OS was not reached. Manufacturing time for axicabtagene ciloleucel was on average 17 days with a 99% success rate.
Safety
The most common adverse reactions reported in the ZUMA-1 trial include cytokine release syndrome (CRS) (94%), fever (86%), hypotension (57%), encephalopathy (57%), tachycardia (57%), fatigue (46%), headache (45%), decreased appetite (44%), chills (40%), diarrhea (38%), and other very common (≥20%) adverse reactions such as febrile neutropenia, infections-pathogen unspecified, nausea, hypoxia, tremor, cough, vomiting, dizziness, constipation, and cardiac arrhythmias.14 The most common (≥ 10%) Grade 3 or higher reactions include febrile neutropenia, fever, CRS, encephalopathy, infections-pathogen unspecified, hypotension, hypoxia, and lung infections. Nearly all patients (>95%) experienced a Grade ≥3 adverse reaction - most frequently anemia, neutropenia, and febrile neutropenia. Axicabtagene ciloleucel carries a boxed warning for CRS and neurologic events as Grade 3 or higher events were observed in 13% and 31% of patients, respectively.12 Axicabtagene ciloleucel is only available through a Risk Evaluation and Mitigation Strategies (REMS) to mitigate the risks of CRS and neurological toxicities.
Guidelines
The NCCN B-Cell Lymphomas guideline recommends axicabtagene ciloleucel as subsequent therapy after second-line therapy for DLBCL, primary mediastinal large B-cell lymphoma or double hit lymphoma.16 Axicabtagene ciloleucel is also recommended as subsequent therapy for patients with histologic transformation to DLBCL after treatment with ≥2 chemoimmunotherapy regimens, which included at least 1 anthracycline or anthracenedione-based regimen, unless contraindicated.
Copanlisib (Aliqopa™)
Indication
Copanlisib received accelerated approval for the treatment of relapsed follicular lymphoma (FL) in patients who have received 2 prior systemic therapies.17,18 The FDA granted orphan drug and fast track designation for copanlisib in the harder to treat third-line setting due to efficacy and safety profiles. Copanlisib’s mechanism of action is novel in that it inhibits mainly phosphatidylinositol-3-kinase (PI3K) alpha and delta isoforms expressed in malignant B-cells. This process causes apoptosis and inhibition of proliferation of malignant B-cell lines. Idelalisib, a first generation PI3K inhibitor, only inhibits a single PI3K-delta isoform.19
Efficacy
The results contributing to the efficacy and safety of copanlisib are only available from the manufacturer and have not been published yet. The approval of copanlisib is based on CHRONOS-1 trial, which was a single-arm, multicenter, phase 2 clinical trial.18 The trial enrolled 142 patients, which included 104 patients with follicular B-cell NHL who have received at least 2 therapies before. All patients were treated with at least rituximab and an alkylating agent in the past. The majority of patients (130/142) received 60 mg of copanlisib on days 1, 8, and 15 of a 28-day cycle. The ORR was 59% (95% CI, 49% to 68%). This medication received accelerated approval based on ORR, which is contingent on the results of a confirmatory trial.
Safety
The most common adverse reactions reported with copanlisib were hyperglycemia (54%), diarrhea (36%), decrease in energy and strength (36%), hypertension (35%), leukopenia (36%), neutropenia, thrombocytopenia (22%), nausea (26%), and lower respiratory tract infections (21%).18 Pneumonia (8%), pneumonitis (5%), and hyperglycemia (5%) were the most frequent serious adverse reactions. Side effects may be different from idelalisib as copanlisib is administered intravenously and bypasses the gastrointestinal (GI) tract in an attempt to minimize severe GI side effects such as colitis. Per the prescribing information, caution is advised for GI toxicity, pulmonary toxicity, hyperglycemia, hypertension, dermatologic toxicity, bone marrow suppression, and infection.
Guidelines
Per NCCN guidelines for B-cell lymphomas, copanlisib is listed as a second-line and subsequent therapy in patients with FL who are refractory to at least 2 prior therapies.16
Durvalumab (Imfinzi®)
Indication
Durvalumab received accelerated approval for the use in patients with locally advanced or metastatic UC who have experienced disease progression with platinum-containing chemotherapy.20,21 The FDA granted priority review and breakthrough therapy designations to durvalumab, and the agent was approved only days before the approval of avelumab, which can be also used in UC. Durvalumab is a monoclonal antibody that inhibits the interaction of PD-L1 with PD-1 and CD80. This mechanism differs from PD-1 inhibitors, as it acts at the ligand on tumor cells. This inhibition leads to the activation of T-cells and decrease in tumor size by allowing T-cells to kill tumor cells. Unlike avelumab, durvalumab is engineered to prevent ADCC. The FDA simultaneously approved the VENTANA PD-L1 assay to test for PD-L1 expression, which may predict the likelihood of response to durvalumab.22
Efficacy
The approval of durvalumab was based on a phase 1/2 open label study.21,23 The study enrolled 191 patients with locally advanced or metastatic UC who have progressed on or refused chemotherapy. Patients received durvalumab 10 mg/kg IV every 2 weeks for up to 12 months, until disease progression, or until unacceptable toxicity. The median follow-up time was 5.78 months and ranged from 0.4 to 25.9 months. The primary endpoint, the ORR, was 17.8% (95% CI, 12.7% to 24%). In patients with high PD-L1 expression, the ORR was 27.6% (95% CI, 19% to 37.5%). The ORR was 5.1% (95% CI, 1.4% to 12.5%) in patients with low or no expression of PD-L1. The median PFS was 1.5 months (95% CI, 1.4 to 1.9 months) with 2.1 months (95% CI, 1.4 to 2.8 months) in patients with high PD-L1 expression and 1.4 months (95%CI, 1.3 to 1.5 months) in patients with low or no PD-L1 expression. The median OS was 18.2 months (95% CI, 8.1 months to not estimable) with 20 months (95% CI, 11.6 to not estimable) in patients with high PD-L1 expression and 8.1 months (95% CI, 3.1 to not estimable) in patients with low or no PD-L1 expression.
Safety
In the clinical study for UC, Grade 3/4 adverse events occurred in 6.8% of patients.23 The most common adverse events were fatigue (19.4%), decrease in appetite (9.4%), diarrhea (8.4%), and rash (7.3%). Immune-mediated warnings and concerns apply, such as adrenal insufficiency, rash, type 1 diabetes, colitis, hepatitis, hypophysitis, pneumonitis, nephritis, and others known to be associated with cancer immunotherapy are listed in the prescribing information.
Guidelines
Per NCCN Bladder Cancer guideline, durvalumab is an option as a subsequent systemic therapy for locally advanced or metastatic bladder cancer after first-line therapy.10
Inotuzumab ozogamicin (Besponsa™)
Indication
Inotuzumab ozogamicin is approved for treatment of adult patients with r/r B-cell precursor acute lymphoblastic leukemia (ALL) which is associated with poor prognosis in adults.24,25 The FDA granted priority review, breakthrough therapy and orphan drug status for this indication associated with poor prognosis. Inotuzumab ozogamicin, an antibody-drug conjugate (ADC) for CD22, selectively binds to tumor cells expressing CD22.25 An internalization of ADC-CD22 complex by cells leads to release of N-acetyl-gamma-calicheamicin dimethylhydrazide, which contributes to double-strand DNA breaks, cell cycle arrest, and apoptosis.
Efficacy
The approval of inotuzumab ozogamicin was based on INO-VATE ALL study.25 This was an open-label, multicenter, randomized, phase 3 study of inotuzumab ozogamicin versus standard of care in 326 adult patients with r/r B-cell ALL (CD22-positive, Philadelphia chromosome (Ph)-positive or negative) requiring first or second salvage treatment.26 The administered dose was 0.8 mg/m2 (or 0.5 mg/m2 if CR or CR with incomplete hematologic response (CRi) was achieved after cycle 1) on day 1, 0.5 mg/m2 on day 8 and 15 of 21 to 28-day cycles. The standard of care consisted of fludarabine with cytarabine and granulocyte-colony stimulating factor, mitoxantrone with cytarabine, or high-dose cytarabine. The primary endpoints were CR and OS. The study showed a higher CR rate in 80.7% (95% CI, 72.1 to 87.7) of patients in the inotuzumab ozogamicin group versus 29.4% (95% CI, 21.0 to 38.8) of patients in the standard therapy group (p<0.001). The PFS was greater at 5 months in the inotuzumab ozogamicin group versus 1.8 months in the standard therapy group with a hazard ratio (HR) of 0.45 (97.5% CI, 0.34 to 0.61; p<0.001). The median OS was 7.7 months in the inotuzumab ozogamicin group versus 6.7 months in the standard therapy group (HR, 0.77; 97.5% CI, 0.58 to 1.03; p=0.04).
Safety
According to the INO-VATE ALL study, the most common non-hematologic adverse event in the inotuzumab ozogamicin was a veno-occlusive liver disease (11% in the inotuzumab ozogamicin group versus 1% in the standard therapy group).26 Common treatment emergent adverse events with inotuzumab ozogamicin consisted of nausea (31%), headache (28%), and pyrexia (32%). The boxed warning for the agent mentions veno-occlusive liver disease and a higher non-relapse mortality after hematopoietic stem cell transplant.25
Guidelines
Per the NCCN ALL guideline, inotuzumab ozogamicin is an option for patients with Ph-positive ALL who are refractory or intolerant to tyrosine kinase inhibitors (TKIs).27 This agent is also recommended in patients with r/r Ph-negative ALL. The guideline also states that inotuzumab ozogamicin is associated with hepatic problems and has an increased risk for post-hematopoietic stem cell transplant non-relapse mortality.
Tisagenlecleucel (Kymriah™)
Indication
Tisagenlecleucel was the first-in-class CAR T-cell therapy.28 Tisagenlecleucel is approved for use following fludarabine and cyclophosphamide lymphodepleting chemotherapy in patients up to 25 years of age with r/r B-cell precursor ALL.29 Tisagenlecleucel targets CD19-expressing malignant cells with genetically modified autologous T-cells encoded with a CAR. Binding of CAR T-cells to CD19 promotes T-cell signaling, expansion, activation, and persistence to eliminate target cells.
Efficacy
Tisagenlecleucel was approved for r/r B-cell ALL based on results from the ELIANA trial.29 The ELIANA trial was an open-label, multicenter, single-arm, phase 2 trial assessing the safety and efficacy of at least 1 treatment of tisagenlecleucel therapy (0.2 to 5.0 x 10^6 cells/kg for patients ≤50 kg or 1.0 to 2.5 x 10^8 cells/kg for patients >50 kg) in 88 enrolled (68 treated) pediatric and young adult patients (median age of 12 years) with r/r B-cell ALL.30 The primary endpoint was overall remission rate of 82.5% with duration of remissions in 64% of patients at 9 and 12 months. The relapse-free probability at 6 months remission onset was 75% (95% CI, 57% to 87%) and OS was not reported. Tisagenlecleucel cellular productmanufacturing failures prevented 7 (8.0%) patients from being treated.
Safety
The most common adverse reactions in the ELIANA trial include CRS (79%), hypogammaglobulinemia (43%), infections (41%), fever (40%), decreased appetite (37%), headache (37%), encephalopathy (34%), hypotension (31%), bleeding (31%), tachycardia (26%), nausea (26%), diarrhea (26%), vomiting (26%), viral infections (26%), hypoxia (24%), fatigue (22%), acute kidney injury (22%), and delirium (21%).30 Half of all patients with CRS in this trial required tocilizumab. The most common (≥ 10%) Grade 3 or higher reactions include CRS, febrile neutropenia, hypoxia, hypotension, increased liver enzymes, decreased appetite, hypokalemia, cytopenias, and neurological events. Two deaths occurred within 30 days of tisagenlecleucel treatment (one due to ALL progression during CRS and another due to cerebral hemorrhage with resolving CRS). Tisagenlecleucel carries a boxed warning for CRS and neurologic events as 49% and 18% of patients experience Grade 3 to 4 effects, respectively. There is a REMS in effect to mitigate the risks of CRS and neurological toxicities.
Guidelines
The NCCN ALL guidelines recommend tisagenlecleucel as a single-agent therapy for patients under 26 years old with r/r B-cell ALL after 2 or more relapses, and if Ph -positive B-cell ALL then also after failure of 2 TKIs.27
Table 1. Properties of newly approved IV oncology agents in 2017.5,12,18,21,25,29,31
Drug Name (Brand) |
Dosage Form(s) |
Dosing and Administration |
Costa |
Avelumab (Bavencio®) |
Single-dose vial; 200 mg/10 mL (20 mg/mL) preservative-free solution for injection |
10 mg/kg IV infusion over 60 minutes every 2 weeks |
$1,832/vial |
Axicabtagene ciloleucel (Yescarta™) |
Single-dose frozen suspension; variable number of cultured, genetically modified cells based on patient-specific weight |
Target dose of 2.0x106 to a maximum of 2.0x108 CAR-positive viable T-cells per kg as IV infusion after completing lymphodepleting chemotherapy on the fifth, fourth, and third day prior to treatment. |
$373,000/autologous cellular treatmentb |
Copanlisib (Aliqopa™) |
Single-dose vial; 60 mg lyophilized powder |
60 mg IV infusion over 60 minutes on days 1, 8, 15 every 28 day-cycle |
$5,040/vial |
Durvalumab (Imfinzi®) |
Single-dose vials; 120 mg/2.4 mL (50 mg/mL) and 500 mg/10 mL (50 mg/mL) solution for injection |
10 mg/kg IV infusion over 60 minutes once every 2 weeks |
120 mg/2.4 ml vial - $1,002/vial 500 mg/10 ml vial - $4,174.57/vial a |
Inotuzumab ozogamicin (Besponsa™) |
Single-dose vial; 0.9 mg lyophilized powder |
IV infusion over 60 minutes on days 1 (0.8 mg/m2), 8 (0.5 mg/m2), and 15 (0.5 mg/m2) of the first 21-day cycle; for subsequent cycles, the dose is 0.5 mg/m2 on day 1 if patients achieved CR or CRi or 0.8 mg/m2 in patients who have not achieved CR or CRi. The doses for day 8 and day 15 are the same as in the first cycle with the exception of subsequent cycles being 28 days long |
$22,440/vial |
Tisagenlecleucel (Kymriah) |
Single-dose frozen suspension; variable number of cultured, genetically modified cells based on patient-specific weight |
0.2 -5.0 x 106 CAR-positive viable T-cells per kg (patients 50 kg and below) 0.1-2.5 x 108 cells per kg (patients above 50 kg) as one infusion 2 to 14 days after completing lymphodepleting chemotherapy |
$475,000/autologous cellular infusionb |
aPricing is based on average wholesale price.
bPricing is based on manufacturer statement.
Abbreviations: CR = complete response; CRi = complete response with incomplete hematologic recovery; IV = intravenous.
Conclusion
This article reviewed 6 novel intravenous or cellular therapies approved in 2017 for at-need patient populations in malignancies such as those with MCC, UC, r/r B-cell lymphoma, ALL, and FL. This represents 33% of all new oncology medications, medication combinations, or biosimilars approved, and 13% of new hematology or oncology indications approved in 2017. As a condition of the accelerated approvals, ongoing clinical trials to confirm clinical benefits of avelumab, copanlisib, and durvalumab are needed. Overall these are much welcomed approvals, but come with significant costs. While exciting breakthroughs in cellular technology such as CAR T-Cell therapy can potentially increase survival, they carry a significant price tag, hospital admissions, and the need for ancillary high cost medications such as tocilizumab. It is yet to be seen how these costs will be weighed against other potential therapies, including stem cell transplants. With combined increases in the complexity of newly approved medications, sky-rocketed price tags, and expedited approval pathways, it has never been more important to advance the conversation that correlates cost with defined value for patients and healthcare systems.
References:
- Number of fast track designation requests granted. Food and Drug Administration website. https://www.accessdata.fda.gov/scripts/fdatrack/view/track.cfm?program=cder&status=public&id=CDER-RRDS-Number-of-Fast-Track-Designations-granted&fy=2012. Updated September 30, 2017. Accessed January 14, 2018.
- CY 2017 CDER breakthrough therapy calendar year approvals. Food and Drug Administration website. https://www.fda.gov/downloads/Drugs/DevelopmentApprovalProcess/
HowDrugsareDevelopedandApproved/DrugandBiologicApprovalReports/
NDAandBLAApprovalReports/UCM494010.pdf. Updated December 31, 2017. Accessed January 14, 2018. - Drugs@FDA: FDA approved drug products. Food and Drug Administration website. https://www.accessdata.fda.gov/scripts/cder/daf/. Accessed January 14, 2018.
- Novel drug approvals for 2017. Food and Drug Administration website. https://www.fda.gov/Drugs/DevelopmentApprovalProcess/DrugInnovation/ucm537040.htm. Updated January 12, 2018. Accessed January 15, 2018.
- Bavencio [package insert]. Rockland, MA: EMD Serono, Inc; 2017.
- FDA grants accelerated approval to avelumab for urothelial carcinoma. Food and Drug Administration website. https://www.fda.gov/drugs/informationondrugs/approveddrugs/ucm557162.htm. Updated May 9, 2017. Accessed January 15, 2018.
- Avelumab (Bavencio). Food and Drug Administration website. https://www.fda.gov/Drugs/InformationOnDrugs/ApprovedDrugs/ucm547965.htm. Updated May 30, 2017. Accessed January 15, 2018.
- Kaufman HL, Russell J, Hamid O, et al. Avelumab in patients with chemotherapy-refractory metastatic Merkel cell carcinoma: a multicentre, single-group, open-label, phase 2 trial. Lancet Oncol. 2016;17(10):1374-1385.
- Patel M, Ellerton J, Infante J, et al. Avelumab in patients with metastatic urothelial carcinoma: pooled results from two cohorts of the phase 1b JAVELIN solid tumor trial. Poster presented at ASCO 2017. J Clin Oncol. 35:6; suppl 330.
- NCCN Clinical Practice Guidelines in Oncology. Bladder Cancer Version 1.2018. National Comprehensive Cancer Network website. https://www.nccn.org/professionals/physician_gls/pdf/bladder.pdf. Published January 8, 2018. Accessed January 8, 2018.
- NCCN Clinical Practice Guidelines in Oncology. Merkel Cell Carcinoma Version 1.2018. National Comprehensive Cancer Network website. https://www.nccn.org/professionals/physician_gls/pdf/mcc.pdf. Published September 18, 2017. Accessed January 8, 2018.
- Yescarta [package insert]. Santa Monica, CA: Kite Pharma, Inc; 2017.
- FDA approves axicabtagene ciloleucel for large B-cell lymphoma. Food and Drug Administration website. https://www.fda.gov/Drugs/InformationOnDrugs/ApprovedDrugs/ucm581296.htm. Updated October 25, 2017. Accessed January 15, 2018.
- Locke FL, Neelapu SS, Bartlett NL, et al. Clinical and biological covariates of outcomes in ZUMA-1: a pivotal trial of axicabtagene ciloleucel (Axi-cel; KTE-C19) in patients with refractory aggressive non-Hodgkin lymphoma (r-NHL). Presented at: American Society for Clinical Oncology Annual Meeting; June 2-6, 2017; Chicago, IL.
- A phase 1-2 multi-center study evaluating axicabtagene ciloleucel in subjects with refractory aggressive non-hodgkin lymphoma (ZUMA-1). Clinicaltrials.gov website. https://clinicaltrials.gov/ct2/show/NCT02348216. Updated December 17, 2017. Accessed February 8, 2018.
- NCCN Clinical Practice Guidelines in Oncology. B-Cell Lymphomas Version 7.2017. National Comprehensive Cancer Network website. https://www.nccn.org/professionals/physician_gls/pdf/b-cell.pdf. Published December 5, 2017. Accessed January 7, 2017.
- FDA grants accelerated approval to copanlisib for relapsed follicular lymphoma. Food and Drug Administration website. https://www.fda.gov/Drugs/InformationOnDrugs/ApprovedDrugs/ucm576098.htm. Updated September 14, 2017. Accessed January 15, 2018.
- Aliqopa [package insert]. Whippany, NJ: Bayer; 2017.
- Zydelig [package insert]. Foster City, CA: Gilead Sciences, Inc.; 2017.
- Durvalumab (Imfinzi). Food and Drug Administration website. https://www.fda.gov/Drugs/InformationOnDrugs/ApprovedDrugs/ucm555930.htm. Updated May 1, 2017. Accessed January 15, 2018.
- Imfinzi [package insert]. Wilmington, DE: AstraZeneca; 2017.
- Roche receives FDA approval for complementary PD-L1 (SP263) biomarker test in urothelial carcinoma. Ventana website. http://www.ventana.com/roche-receives-fda-approval-complementary-pd-l1-sp263-biomarker-test-urothelial-carcinoma/. Updated May 2, 2017. Accessed February 12, 2018.
- Powles T, O'Donnell PH, Massard C, et al. Efficacy and safety of durvalumab in locally advanced or metastatic urothelial carcinoma: updated results from a phase 1/2 open-label study. JAMA Oncol. 2017;3(9):e172411.
- FDA approves inotuzumab ozogamicin for relapsed or refractory B-cell precursor ALL. Food and Drug Administration website. https://www.fda.gov/Drugs/InformationOnDrugs/ApprovedDrugs/ucm572133.htm. Updated August 17, 2017. Accessed January 15, 2018.
- Besponsa [package insert]. Philadelphia, PA: Pfizer; 2017.
- Kantarjian HM, DeAngelo DJ, Stelljes M, et al. Inotuzumab ozogamicin versus standard therapy for acute lymphoblastic leukemia. N Engl J Med. 2016;375(8):740-753.
- NCCN Clinical Practice Guidelines in Oncology. Acute Lymphoblastic Leukemia Version 5.2017. National Comprehensive Cancer Network website. https://www.nccn.org/professionals/physician_gls/pdf/all.pdf. Published October 27, 2017. Accessed January 8, 2018. In.
- FDA approves tisagenlecleucel for B-cell ALL and tocilizumab for cytokine release syndrome. Food and Drug Administration website. https://www.fda.gov/drugs/informationondrugs/approveddrugs/ucm574154.htm. Updated September 7, 2017. Accessed January 25, 2018.
- Kymriah [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corporation; 2017.
- Buechner J, Grupp S, Maude S, et al. Global registration trial of efficacy and safety of CTL019 in pediatric and young adult patients with relapsed/refractory (R/R) acute lymphoblastic leukemia (ALL): update to the interim analysis. Clin Lymphoma Myeloma Leuk. 17:S263-S264.
- LexiComp [database]. Hudson, OH: Wolters Kluwer Health; 2018. https://online.lexi.com/lco/action/home. Accessed January 5, 2018.


Contents
Columns
Educational Affairs Meeting News
Professional Affairs - Call for Entries
Features
You Want Me to Talk to a Legislator???
College Connection
Midwestern University Chicago College of Pharmacy
Roosevelt University College of Pharmacy
More
Officers and Board of Directors
ICHP Pharmacy Action Fund (PAC) Contributors
Regularly Scheduled Network Meetings
Chicago Area Pharmacy Directors Network Dinner
3rd Thursday of Odd Months
5:30pm
Regularly Scheduled Division and Committee Calls
Executive Committee
Second Tuesday of each month at 7:00 p.m.
Educational Affairs
Third Tuesday of each month at 11:00 a.m.
Government Affairs
Third Monday of each month at 5:00 p.m.
Marketing Affairs
Third Tuesday of each month at 8:00 a.m.
Organizational Affairs
Fourth Thursday of each month at 12:00 p.m.
Professional Affairs
Fourth Thursday of each month at 2:00 p.m.
New Practitioner Network
Second Thursday of each month at 5:30 p.m.
Technology Committee
Second Friday of each month at 8:00 a.m.
Chicago Area Pharmacy Directors Network Dinner
Bi-monthly in odd numbered months with dates to be determined. Invitation only.